Using accurately defined latency periods of various cancers to inform possible effects on incidence trend rates of both sunshine stored vitamin D after good summers and changes to the radio frequency environmental background. By Dr Chris Barnes, Bangor Scientific and Educational Consultants, Bangor, Gwynedd, Wales, UK. E-MAIL doctor.barnes@univ.bangor.ac.uk
Dr Barnes Homepage http://www.drchrisbarnes.co.uk
Abstract
Accurate cancer latency periods established from the effect of the Chernobyl accident on UK Cancer incidence trends are used to explore the effects of both sunshine ( serum vitamin D) and changes to the radio frequency environmental background on such incidence trends. The effects of serum vitamin D found in a previous World study by geographic metal analysis due to the author are confirmed. Vitamin D is shown to be cancer protective in several cancers and it is believed uniquely, a link between good summers and general cancer protection has been identified. It is believed that serum vitamin D plays an essential role. Predictions in global dimming suggest Europe may now be entering a brightening phase. Provided UVB brightens in line with the general prediction for solar irradiance, serum vitamin D shortage in Britain may once again become a thing of the past. In this respect we ought to see a knock on effect in a reduction of all the vitamin D sensitive cancers quite shortly but of course dependent on latency. Another tier of reinforcement to the many findings of this and other authors to the notion that RF radiation is not good for a certain section of the population and is associated with increased risk of more than one type of cancer. It would appear DVB is almost as potent as the old style VHF analogue TV and more potent than UHF analogue TV when all incidence trends for the three cancers concerned are taken into account. A surprise result is for TETRA, which shows either a flattening of the increase or even a slight trough for NHL. Some potential reasons for this are discussed although further work is also proposed. Finally there is some suggestion that 3G might be about to become a potent cancer producer this is unexpected based on one of the author's prevoius hypotheses and the jury remains out.
Introduction
Cancer latency is the period between carcinogenesis when the first few cancer cells form to the period when the cancer presents as a tumour sufficiently large to be felt by palpation, or if it is inaccessible to palpation then for it to be large enough to show up on body imaging scans (1) .
Cancer latency is of interest for various reasons. Firstly, because it is linked inversely to tumour proliferation rate, see Olsson et al 2003 (2) . Secondly, because it is linked to detection , see Koenty (2005) (3) and Benoit (1995). Thirdly, for some cancers such as mesothelioma it is related to initial exposure and to lifespan (4)
To the present author, it would seem obvious that cancer latency would be related to the promoter as well as to the initiator, see for example Barnes' 2013 study on TV emissions and pollution (5), http://drchrisbarnes.co.uk/Cancer%20Epidemiology.html but despite this there is relatively little in the literature on similar matters. The two notable exceptions are Ewing et al (1988)(6) who show that for mouse skin tumour progression both initiator and promoter concentrations can influence tumour progression rates. Wong (2003) also shows that mixed hormonal promoters shorten rat breast tumour progression rates.
It would seem that minimum latency periods are observed when there is human exposure to a very aggressive mixture containing both initiators and promoters. A tragically sad, yet almost unique opportunity to follow such an event was due to the dust inhaled by some persons when the world trade towers in New York came down, so called 9.11. Howard, (May 2013) has given a revision of his recent White Paper on 9.11 showing the minimum expected latency periods for a variety of cancers (7).
Another even that effected the whole world but Ukraine and parts of Europe and Britain very badly was the Chernobyl nuclear accident in 1986. Due to the Easterly winds and unusual direction of weather systems at the time, Britain was effected a day or two later by radioactive rain containing mainly radioactive Caesium and Iodine.
Ionising radiation from the Chernobyl fallout would have been a remarkably good and consistent tumour initiator for an exposed and susceptible section of the public no matter how small by either inhalation or ingestion of polluted water, milk, vegetables or meat.
The present author, Barnes, has shown in a very recent publication that the effects of the Chernobyl incident show up as a positive going blip in the UK cancer versus time trend statistics for at least seventeen different cancers (8) . The initiation or rising edge of this blip yields the minimum latency time a particular type of cancer and the falling edge should yield the maximum time. Fortunately, Cancer Research UK website has published data on all sorts of cancers trends against time.
Hypothesis and Methodology
Leukaemia has a particularly short latency period and thus any environmental change of known date which is thought to have a pro-cancer or anti-cancer effect ought to make itself known in the weighting of the leukaemia time trend rate. In the previous paper (8) , Chernobyl was used as a calibration aid to establish this phenomenon. The trend rate between 1975 and 2010 is published in the UK by the charitable organisation Cancer Research UK.
In another paper using geographic meta-analysis (Barnes )(9) associations have been established between the prevalence of various cancers and the degree of penetration of wireless technology. The author has coined the phrase 'RF cancers' to describe the ones which seem to show the most significant association. Similarly in that paper the protective effects of melatonin and vitamin D were also explored on a geographic basis; night light pollution being equated with lowered melatonin levels and increased solar U/V levels being associated with increased serum vitamin D levels. Some results of that study (9) are shown below, together with a third column which is the ratio of RF:Vit D effect, see table 1 below:
|
Type |
RF |
Low u/v/Vit D |
Ratio RF/VITD |
|
|
|
|
|
|
Bowel |
0.82 |
0.76 |
1.07 |
|
Brain/nervous |
0.74 |
0.64 |
1.15 |
|
Breast |
0.9 |
0.75 |
1.2 |
|
Hodgkin Lymp |
0.81 |
0.83 |
.98 |
|
Kidney |
0.69 |
0.76 |
.91 |
|
Leukemias |
0.74 |
0.73 |
1.01 |
|
Lung |
0.58 |
0.7 |
.82 |
|
Melanoma |
0.64 |
0.28 |
2.28 |
|
Myeloma |
0.79 |
0.41 |
1.92 |
|
Prostate |
0.8 |
0.64 |
1.25 |
|
Table 1 |
|
|
|
All the cancers on the list have a statistically significant correlation with wireless penetration, and all are significantly protected against by vitamin D with the exception of Melanoma and Myeloma.
It is proposed to use this knowledge with regard to vitamin D to test the present hypothesis. The best and sunniest summers in the period 1975 to 2010 have been those of 1976, 1991, 1995 and 2006. Therefore it is proposed that there should be found a drop in the relevant cancer incidence rates after the time of each relevant latency period after each of these successive dates. On the basis of the above, Non- Hodgkin lymphoma ought to show the best improvement after good summers i.e. after serum vitamin D improvement. On the other hand Melanoma should indicate changes in the radio frequency environment without being overly sensitive to good summers ( vitamin D). Leukaemia should be a function of both. Breast should be a function of both and Prostate ought to behave very similarly to breast allowing for the longer latency period.
Assuming this can be shown, the hypothesis predicts that changes in the rate for other environmental factors should be able to be assessed accordingly. The main other environmental factor of interest to the present author is the radio frequency emission background to which the population are exposed.
Data sets
The data sets are essentially those published on the Cancer Research UK website.
Results and Discussion
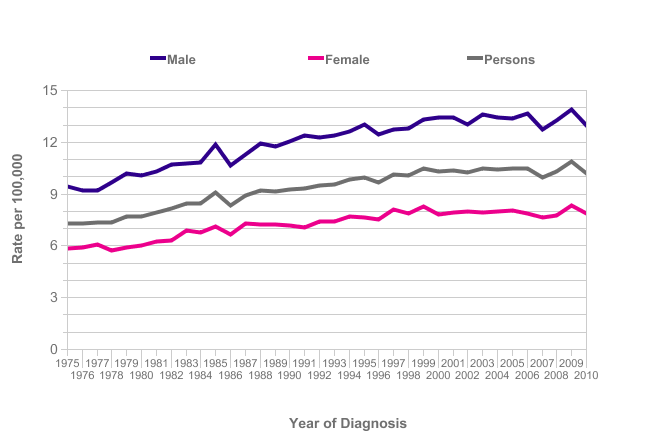
Figure 1 Leukaemia
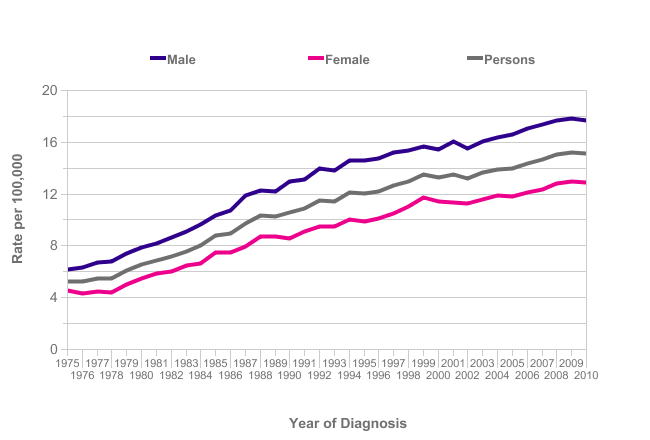
Figure 2 Non -Hodgkin Lymphoma
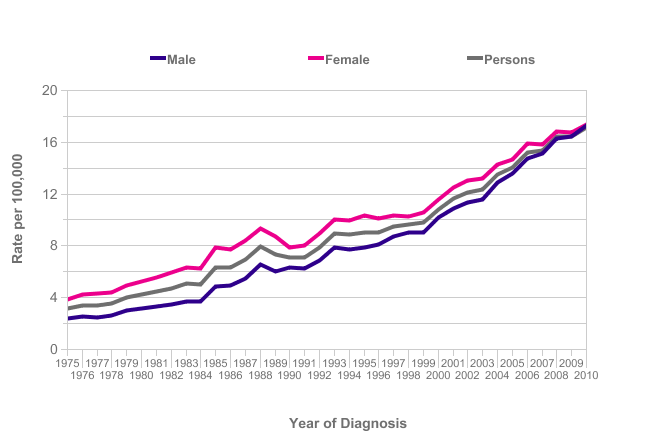
Figure 3 Melanoma
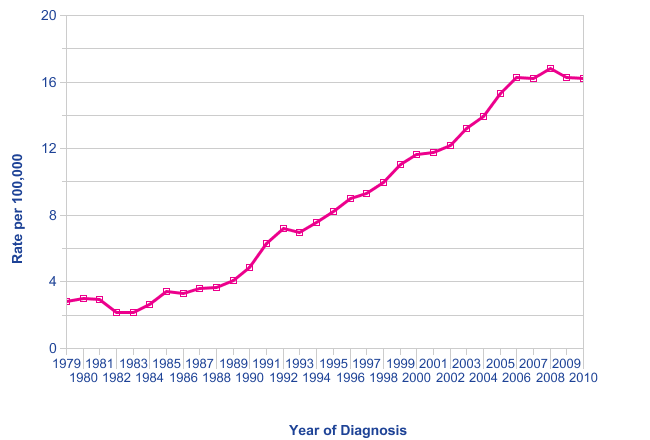
Figure 4 In situ breast cancer
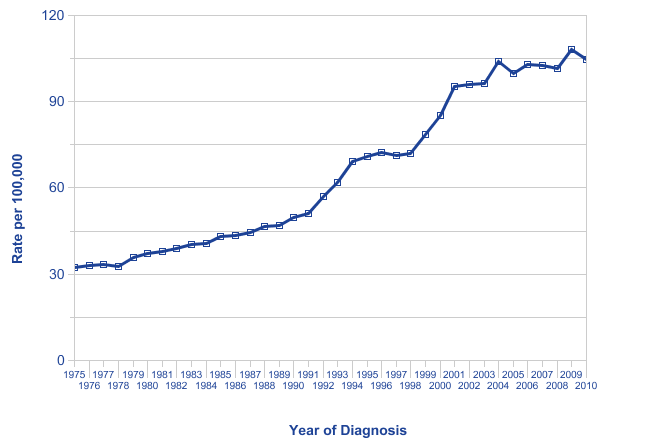
Figure 5 Prostate Cancer
The results in terms of environmental effect of good summers ( serum vitamin D production) are exactly as predicted. Leukaemia with the shortest latency shows a levelling out of the generally increasing trend in 1977, 1992 and 1996 and a trough at 2007. All these are about a year after very sunny summers and are exactly as expected and confirm the hypothesis in this respect. NHL shows similar but more pronounced effects to Leukaemia at these dates again, exactly as predicted.
Melanoma shows less effect at these dates but shows a generally steeper increase in line with the ever increasing levels of RF radiation to which people are exposed.
Breast cancer has been shown previously by Barnes (2013)(8) to have a 7 year latency with respect to Chernobyl. Assuming this latency applies generally, yields some interesting and exciting results. Distinct troughs can be seen at 1983, 1998 and 2002 which are each seven years after the high vitamin D yielding summers of 1976,1991 and 1995.
For prostate cancer the corresponding features are also present but delayed by a further four years. This is again exactly as expected on the basis of the shortest latency period recently identified by Barnes for Prostate cancer in the UK which is 11 years (I.e. 7+4).
The search for effects due to background changes in environmental RF radiation .
Because key dates are known when the UK made changes to various aspects of television, radio and mobile phone broadcasting, then if there is cause and effect, one should be able to search the form of the cancer incidence data trend lines for evidence of such effect. Further according to the present hypothesis and evidence from the previous world study geographic meta-analysis study (9) the evidence should be stronger in some cancer trends than others.
There have been an enormous number of changes made to background electromagnetic pollution in the last six decades with an ever expanding use of the UHF and microwave spectrum especially over the last two decades. Human kind have evolved for millennia attuned only to natural electromagnetic radiation due to earth magnetism, lightening storms and space weather. Man is an electromagnetic animal ( see Smith and Best ISBN 0-460-86044-5)(10) and it goes without saying that all these transmission frequencies would be expected to have some effect.
The main changes made in the electromagnetic spectrum at National level since 1969 are as follows :
1969 UHF TV turned on
1985 VHF TV turned off
1988 Analog mobile phones
1990 Experimental DAB
1993 GSM 900 2G mobile phones
1995 DAB Launched
1997 Channel 5 analogue UHF launched
1998 Experimental DVB
2000 TETRA Police Radio System Launched
2002 DVB Launched
2004 3G Launched more use of 1800 MHz GSM and 2100 MHz UTMS
2008,9,10 Some UHF Analogue TV off
2012 All UHF Analogue TV off.
Clearly this is a formidable list of changes with an almost apparently increasing frequency of events. The predictor is that in all but cancers with the very shortest latency it may be impossible to see trend line changes for all these changes in the radio frequency environment as some may be smeared within a latency period. Of the cancers considered herein and generally, Leukaemia and NHL have very short latency periods and it should be possible to resolve individual effects but with cancers such as Breast cancer with a 7 year latency period the prediction is that not every single effect may be wholly resolvable.
There is of course a considerable volume of data to analyse yet for the appearance of trends this can most easily be done by visual inspection. At the end of the day the human vision system and brain, its neural network is a superb pattern recogniser and classifier.
The author has attempted to impart a meaningful interpretation of the results in the following table where initially just three cancers have been considered these are Leukaemia; NHL and In-situ Breast:
The largest observable change is seen to occur in 1985 when VHF TV Broadcasting was switched off. VHF TV Broadcasting employed frequencies in two bands called Band I ( 48-66 MHz and Band III ( circa 180-210 MHz). Video modulation was Vestigial Side-band a sort of amplitude modulated emission and audio modulation was FM. Line and Frame synchronisation pulses were also emitted. The changes which are most likely in association with the VHF TV switch off are quite pronounced and are almost step functions as would be expected. No other environmental or meteorological change has been found which could account for the fall in these cancer incidence rates. Leukaemia and NHL have previously been shown to have very short latencies and are thus ideal for these cause and effect type of investigations. When VHF TV was switched off Leukaemia incidence fell by 20%, the increase in NHL stopped and the incidence rate was level and after the appropriate 7 year latency ( 7) the In-situ Breast cancer rate fell by 8 %.
Cancer rates are seen to increase again step wise after 1986 in part due to the Chernobyl accident which has been discussed by the present author elsewhere (8) and for Thyroid cancer by others (11).
Leukaemia has previously been associated with both RF emissions and ELF electromagnetic fields. It has been suggested that the frame synchronisation pulses in analog TV emissions may aggravate their adverse bio-effect (12). Propagation attenuation of these lower VHF frequencies is not so high as for UHF so people would have also been exposed to higher average field strengths. The head and body are also resonant as dielectric resonators close to these frequencies so it is easy to see why removing them had such a profound effect on the cancer incidence rates.
After the spike in Leukaemia and NHL incidence rates thought to be due to the Chernobyl incident a levelling out of the incidence rate is noted until 1989 for Leukaemia and 1990 for NHL. A corresponding levelling is noted for In-situ Breast cancer some 7 years later between 1996 and 1997. This delay is to be expected because the true statistically effect cannot show until the minimum latency period is worked through. Although the concept of relapse free survival rates seems to have been dealt with by Cotterill et al (2000)(11) for Chernobyl related Thyroid cancers they seem, perhaps somewhat surprisingly, to have overlooked the fundamental principle of needing to have latency period in incidence break point calculations.
After these plateaus a whole series of important and fundamental changes to the background RF pollution environment in Britain commenced. As predicted with fast the two fast latency rate cancers considered, namely; Leukaemia and NHL, it has been possible to attach cause and effect to individual events whereas for Breast cancer the changes in RF environment between 1988 and 1995 although causing a substantial 20% increase in the cancer incidence rate cannot readily be separated because of the minimum 7 year latency period.
It is very informative to look at the two cancers which show separable cause and effect for the introduction of analogue mobile phones, some GSM 900 MHz mobile phones and some DVB. For both cancers, analogue mobile phones showed the biggest single increase, 10 % for Leukaemia yet only 3% for NHL, with correspondingly less increases for the other technologies. However, the rise was very steep when most DVB was introduced into the UK 1997. Lauer (13) has commented on the potency of DVB to disturb the immune system and has showed effects in the French cancer incidence data. The early mobile phone technologies showed an inseparable effect in the available Breast cancer incidence trends but each introduction of DVB showed steep rises of 7% and 6% respectively. It is clearly potent.
3G uses a mix of technologies so that some GSM (TDMA) and CDMA modulation will still be being used more predominantly on 1800 MHz UMTS for mobile internet being predominantly used on 2100 MHz The cell phones used with 3G are predominantly a mix of GSM and UMTS whereas the base stations transmit one or the other. 3G was first offered in the UK in 2001 but was not widely adopted until 2004. Thus 2004 was taken as the effective date for this present study.
The effect of 3G appears to be an 8% rise in Leukaemia and a 5% rise in NHL. Due to the longer latency period it is impossible to comment on breast cancer.
Finally between 2008-2010 some UHF analogue TV transmitters were turned off. The effect seems to have been slight falls in Leukaemia and NHL but not as significant as when VHF was turned off. It is too early to comment on the effect for breast cancer.
Conclusions
Firstly, this work has shown, it is believed uniquely, to identify a link between good summers and general cancer protection. It is believed that serum vitamin D plays an essential role. It confirms the findings of an earlier world study using geographic meta-analysis. Predictions regarding changes in global dimming tend to suggest Europe may now be once again entering a brightening phase, except for those living under major air corridors. Provided UVB brightens in line with the general prediction for solar irradiance, serum vitamin D shortage in Britain may once again become a thing of the past. In this respect we ought to see a knock on effect in a reduction of all the vitamin D sensitive cancers quite shortly but of course wholly dependent on latency.
Secondly, this present work adds yet another tier of reinforcement to the many findings of this and other authors to the notion that RF radiation is not good for a certain section of the population and is associated with increased risk of more than one type of cancer. What a finding like this cannot confirm is the bio- mechanics of this risk but this has been discussed elsewhere and is essentially thought to be a combination of genotype and physical location which may be determined by a very specific quantum mechanical argument.
Thus there is no need for RF to be a direct carcinogen for it to be dangerous it can be a promoter acting with natural or anthropogenic ionising radiation or with chemical carcinogens. Smith and Best (10) have, however, explained how by the imprinting of biological water RF and chemical molecules can both leave equivalent imprints. Another potential mechanism as yet unexplored is the action of RF on the pineal gland. It is hoped to report on this in the near future.
Due to the above and due to the different information carried and imparted if one accepts quantum mechanics plays a part in both time and space for the RF bio-interaction then the bio-damage will depend not only on the frequency of the RF but on the modulation scheme employed as well (13). For instance it would appear DVB is almost as potent as the old style VHF analogue TV and more potent than UHF analogue TV when all incidence trends for the three cancers concerned are taken into account.
Thirdly a surprise result is for Tetra, which shows either a flattening of the increase or even a slight trough for NHL. Tetra uses π/4 DQPSK (Differential Quaternary Phase Shift Keying, phase shifts of π/4) and an access scheme using TDMA (time-division multiple access) TDD/FDD (time and frequency division duplex). Some have suggested that Tetra ought to be biologically dangerous due to the 4 time slots per TDMA frame (56.67 ms) 14.167 ms per time slot containing 255 symbols, BCCH in time slot 1 giving equivalent pulse repetition frequencies of approximately 70 Hz and .98 Hz for the base stations and 17.64 Hz for the handsets. Clearly, at least for the moment this does not seem to be borne out in the statistical cancer incidence records. Although TETRA features in 3 out of 17 cancers in a recent study defining key distances form transmitter masts, 2 of these were also at critical distances from 900 MHz GSM emitters and it looks as though it is the GSM that is the problem here. It is intriguing that TETRA ( at a distance) i.e. Base Stations may actually have an anti-cancer effect. 70 Hz is very close to the 9th Schumann resonance. Schumann resonance is known to have an invigorating effect on the immune system. On the other hand adverse effects have been reported by users of the handsets. Clearly, further work is urgently needed here.
Finally there is some suggestion that 3G might be about to become a potent cancer producer this is unexpected based on one of the author's previous hypotheses and the jury remains out.
References
Olsson (2003) http://www.biomedcentral.com/1471-2407/3/11
Ewing et al 1988http://cancerres.aacrjournals.org/content/48/24_Part_1/7048.full.pdf
Howard http://www.cdc.gov/wtc/pdfs/wtchpminlatcancer2013-05-01.pdf
Barnes (2013) http://www.drchrisbarnes.co.uk/Chernobyl1.html
Barnes (2013) http://www.drchrisbarnes.co.uk/World.htm
'Electromagnetic Man' Smith and Best ISBN 0-460-86044-5
Cotterill et al (2001)http://javali.fcav.unesp.br/sgcd/Home/departamentos/morfologia/ELISABETHCRISCUOLOURBINATI/materialdidatico/rad-5-cancer-de-tireoide-em-criancas-depois-de-chernobyl.pdf
Lauer (2013) http://hal.archives-ouvertes.fr/docs/00/87/72/98/PDF/publiarx.pdf