Using geographic meta-analysis to ask are Radio
Frequency (RF) Technology Advances the Smoking Gun for World cancer
increases? By Dr Chris Barnes e-mail
doctor.barnes@univ.bangor.ac.uk
Dr Barnes Homepage http://www.drchrisbarnes.co.uk
Abstract
Wireless technology has advanced relentlessly over the
last two or so decades and now pervades the daily lives of virtually every
individual in the developed World. Even in developing countries penetration is
ever increasing and only the remotest parts of the World are now without any
coverage at all. World cancer statistics
are used not only to enhance the cancer by cancer correlation on the basis of a
wider gene pool but also to perform geo-spatial meta-analyses against GSM
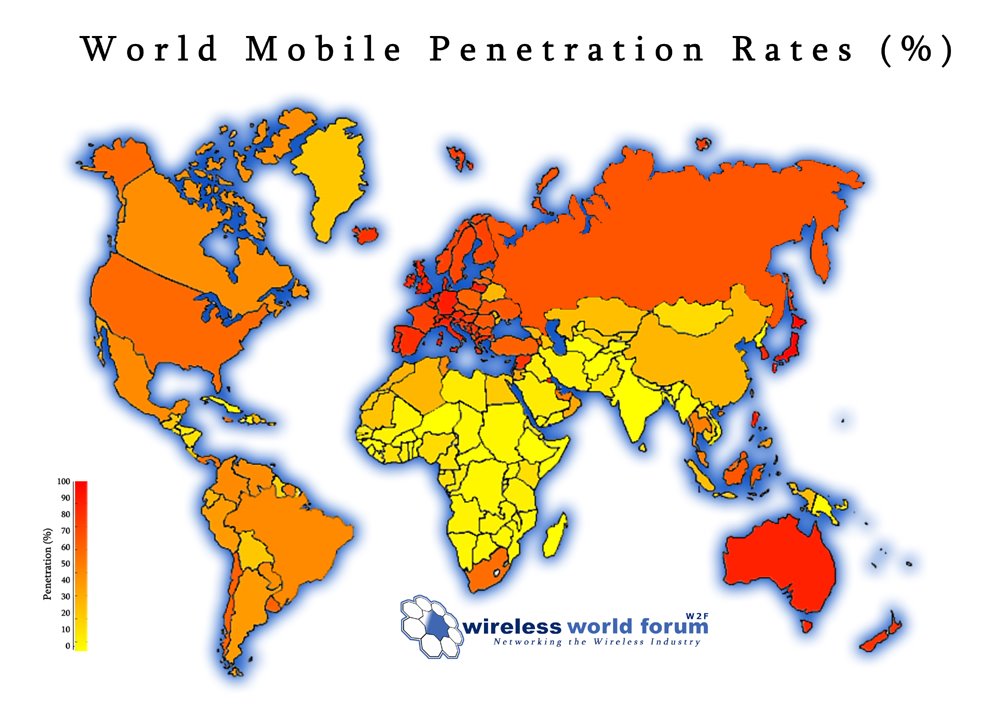
penetration (a good indicator of RF technology advancement and signal coverage
area). Other reasons have recently been cited for abundance of specific cancers
in some reasons of the world and lack of in others and these are explored, for
example, lack of Vitamin D due to low sunlight levels is one possibility. Vitamin D has recently been acknowledged as
having anti-cancer protective properties.
It has also been proposed that the hormone melatonin may protect from
some cancers, thus less cancer might be expected in areas of the world with
less night-time light pollution. What is
clear is that no study can ever have a larger cohort than the entire number of
cancer cases in the world. It is
suggested that this study provides the strongest and undeniable associative
evidence yet of the use of
RF technologies and cancer, especially for Breast Cancer.
Introduction
Wireless technology has advanced relentlessly over the last two or so decades and now pervades the daily lives of virtually every individual in the developed World. Even in developing countries penetration is ever increasing and only the remotest parts of the World are now without any coverage at all.
,
Of course in some parts of the world humans have been exposed to radio waves of various intensities since the dawn of broadcasting and particularly so since TV broadcasting began in earnest after WW2.
Radio frequencies at high levels and in direct contact with humans cause obvious damage such as burns as currents flow in tissues. The big question asked over the last three or four decades has been are there any dangerous non-thermal effects of Radio Frequency Radiation?
There have been numerous in vitro and animal studies of the effects of RF at least 60% of which seem to show bio-effects and bio-damage suggesting that RF could possibly be carcinogenic but if not it could be ,at least, a cancer promoter.
There have also been a handful of epidemiological studies mainly on the effects of TV broadcasting and one German study on the effects of mobile phone base stations. Such studies again have produced mixed results which vary from very weak associations of RF with certain types of cancers to much more certain associations with significant relative risk values, if in single figures.
Occupational risk has also been
assessed for various groups who use RF such as maintenance and repair
engineers, radio amateurs and ship’s radio operators but again quite low
relative risk figures have been returned, generally in the range 1.3-3, see for
example Thomas et al [1] and Hitchcock [2]. From an occupational perspective
radio, electronic and electrical engineers may also be exposed to a variety of
other potential hazards which could include carcinogens such as fumes solvents and
oils, see Occupational
Cancers
edited by Sisko Anttila, Paolo Boffetta [3].
Perhaps because of the above and perhaps because of resistance from network operators the licensing and safety authorities of Western Countries have not been persuaded to reduce Human Exposure limits for RF radiation despite substantial safety lobbies from a number of well-known and concerned scientists.
Meta-analysis is a very powerful technique which other than by the present author does not appear to have been used in attempting to evaluate RF hazard.
Very recently indeed, I have employed meta-analysis on the relationship between the growth of different cancers in the UK and the growth in TV Licensing since the 1950’s [4].
For a number of cancers, which were Breast, Leukaemia, Prostate and Brain, deemed by Barnes as ‘RF’ cancers their growth linear regression function with growth in TV licenses issued since 1947 is close to unity. This shows an indisputable association, with a relative risk of developing an ‘RF’ cancer such as breast or leukaemia some 5 times higher at present than in 1947. A complication with these results is that I had to make the assumption, perhaps perfectly reasonable, that as number of television license subscribers increased then so did transmitter coverage area and hence RF exposure per individual.
Also in the same study I showed using
Polynomial analysis shows Western cancer rates, US and UK now to be slowing
down but still elevated. I discussed two
possible reasons for this. One could be
that the television sets themselves when CRT based were seriously aggravating
the cancer statistic. There are three
perfectly plausible reasons why this should be which are; indoor pollution, ELF
EMR and X-Radiation. The second
plausible reason might be that as RF technologies saturate then so will the
cancer statistic possibly because there
is no longer one dominant pulse rate or modulation scheme so the RF overall
looks ‘noisier’. Biological systems
often function well in the presence of noise, this is the so called principle
of stochastic resonance, see for example McDonnell and Ward [5], Hanggi
(2002) [6], Levin
and Miller (1996) [7], Weisenfield and Moss [8],
and is inherent to genetic systems, see Gonze (2002) [9].
In 2013, I also revaluated
reports of excess Childhood and Adult cancers along the Menai
Straits, previously ascribed to be due by the original authors to Nuclear Radiation
form coastal silt. Other than
retinoblastoma all the other cancers reported could have different and possibly
multiple associations which would account for the excesses observed. I showed that the spatial distribution of
relative risk for all cancers in Bangor, Caernarfon and Colwyn
Bay can equally and alternatively be accounted for by considering relative
distance from the most powerful TV transmitter at Llandonna. There is fierce disagreement amongst
scientists as to whether radio
frequency radiation (RFR) is a cancer initiator or carcinogen per se but it is
easier to see how it could be a promoter [10].
Most cancers with the exception of liver and cervical cancers are known to occur at significantly lower rates in developing countries. Furthermore many developing countries did not have TV broadcasting until at least the 1980’s and even today some just use satellite reception. However in recent years mobile operators and mobile internet providers are investing heavily into increasing penetration into developing countries. There are however, still significant regions of the World with little or no penetration of Wireless technology and if the hypothesis that RF is associated with cancer is correct then these should be the regions with least incidence.
In the past I have shown cancer to cancer incidence association for certain types of cancer in the UK and have deemed and named these to be ‘RF’ cancers. Such an association is also suggestive of a common mode of interaction possibly meaning only persons with a particular genotype or set of genetic mutations might be susceptible to RF cancers?
Using World cancer statistics not only should it be possible to enhance the cancer by cancer correlation on the basis of a wider gene pool but also it should be very readily possible to perform geo-spatial meta-analyses against GSM penetration (a good indicator of RF technology advancement and signal coverage area).
Other reasons have recently been cited for abundance of specific cancers in some reasons of the world and lack of in others. Lack of Vitamin D due to low sunlight levels is one possibility. Vitamin D has recently been acknowledged as having anti-cancer protective properties, see for example Deeb et al (2007) [`11].
It has also been proposed that the hormone melatonin may protect from some cancers, thus less cancer might be expected in areas of the world with less night-time light pollution, see for example E S Schernhammer1,2 and K Schulmeister (2004) [12]. Note there are some 50 other major publications in this area.
Data Sets
All the data sets used were taken straight from the public domain. The most up-to-date World cancer incidence statistics are those for 2008 and these were taken from ‘Cancer Research UK’ website. GSM penetration maps were taken from ‘Wireless World Forum 2006’. World solar U/V mapping with figures was also obtained. World night sky light pollution mapping with figures was obtained from http://www.lightpollution.it/worldatlas/pages/fig1.htm.
The geographic mapping for these data sets is shown below.
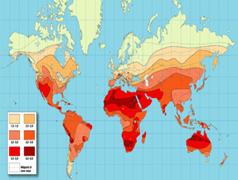 Solar U/V
Solar U/V
 Night
light pollution from http://www.lightpollution.it/worldatlas/pages/fig1.htm
Night
light pollution from http://www.lightpollution.it/worldatlas/pages/fig1.htm
Results
The correlations of various world cancer incidence versus RF Wireless penetration percentage, versus Vitamin D deficiency and versus Melatonin deficiency were evaluated using linear correlation software routines and have been summarised as an XL file given in figure 1 below:
|
Type |
RF |
Low u/v/Vit D |
High night light/melatonin def. |
|
Bowel |
0.82 |
0.76 |
0.59 |
|
Brain/nervous |
0.74 |
0.64 |
0.56 |
|
Breast |
0.9 |
0.75 |
0.7 |
|
Hodgkin Lymp |
0.81 |
0.83 |
0.56 |
|
Kidney |
0.69 |
0.76 |
0.75 |
|
Leukemias |
0.74 |
0.73 |
0.66 |
|
Lung |
0.58 |
0.7 |
0.6 |
|
Melanoma |
0.64 |
0.28 |
0.24 |
|
Myeloma |
0.79 |
0.41 |
0.39 |
|
Prostate |
0.8 |
0.64 |
0.7 |
Figure 1
With the exception of lung cancer, commonly known to be strongly associated with use of tobacco products, all the other cancers investigated seem to have a large association with RF, particular Breast cancer. The cancers which appear to be least protected by vitamin D and melatonin are highlighted in yellow and are Melanoma and Myeloma. The notion of strongly correlating ‘RF’ cancer with another strongly correlating ‘RF’ cancer is tested by correlating World Breast and Bowel cancer incidence, see figure 2 below:
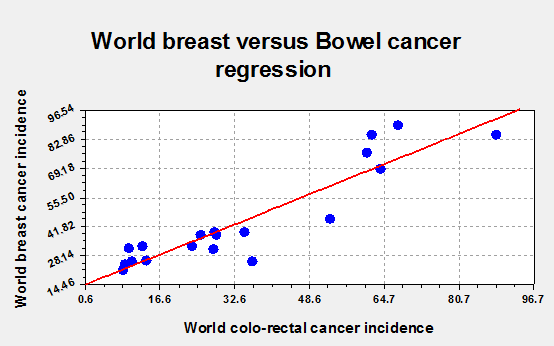
Figure 2.
The linear regression in figure 2 is .92 which is highly significant. Indeed with r=.92 and 17 degrees of freedom, the two-tailed P value is less than 0.0001. By conventional criteria, this difference is considered to be extremely statistically significant. A common potential mechanism which could potentially account for this would be the inactivation of various tumour suppressor genes, see for instance Herman et al (1995) [13] or the presence of mutant p53 gene, see Levine et al (1994) [14].
Discussion
Relative risks for various ‘RF’ cancers vary between 4.5 and 11 taking the age standardised incidence figures in areas of the world with 100% wireless penetration compared with areas of the world with no penetration. These risk factors are comparable with the values I obtained for ‘TV use’ in the UK and with values obtained by Cherry (2002) in the Sutro TV tower study [15].
Risk can of course in some cases be multiplicative. For instance it may be that only part of this risk comes from exposure to actual wireless signals from transmitting base stations and another part comes from exposure to the associated hardware that goes with mobile phone and internet use such as power supplies, chargers VDU’s and computers, all of which provide ELF fields with alleged risks of their own.
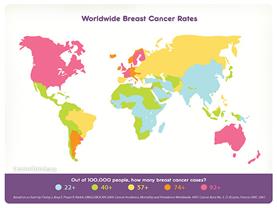
What is clear is that no study can ever have a larger cohort than the entire number of cancer cases in the world. It is suggested that this study provides the strongest and undeniable associative evidence yet of the use of RF technologies and cancer, especially for Breast Cancer, see mapping below:
The study also shows a significant correlation between vitamin D deficiency and cancer. This holds out hope that some cancers may in future be treatable by oral or topical administration of vitamin D and/or by exposure to UV/B lighting. Melatonin seems less significant than vitamin D with the exception perhaps of Breast, Kidney and Prostate Cancer and Leukaemia.
Further work.
It is hoped and expected that these results will give molecular geneticists more insight into the precise nature and mechanisms of these particular cancers. Some of the cancers which the present author has labelled ‘RF’ cancers are also readily initiated in some individuals by ionising radiation. It is hoped to discuss the link elsewhere.
References
1.
http://www.ncbi.nlm.nih.gov/pubmed/3474455
4.
http://www.drchrisbarnes.co.uk/Meta.html
5.
http://www.nature.com/nrn/journal/v12/n7/full/nrn3061.html
6.
http://www.csc.matco.ro/atl2006/documentatie/teorie/10_RS_biologie_general.pdf
7.
http://www.ncbi.nlm.nih.gov/pubmed/8600392
8.
http://phstudy.technion.ac.il/~wn116029/references/Project%20No.18/Wiesenfeld.pdf
9.
http://homepages.ulb.ac.be/~dgonze/HOUCHES/noiseA.pdf
10. http://drchrisbarnes.co.uk/Cancer%20Epidemiology.html
11. http://www.nature.com/nrc/journal/v7/n9/abs/nrc2196.html
12. http://www.nature.com/bjc/journal/v90/n5/abs/6601626a.html
13. http://cancerres.aacrjournals.org/content/55/20/4525.short
14. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1968876/
15. https://researcharchive.lincoln.ac.nz/bitstream/10182/3969/1/90_r3_EMR_Sutro_Paper_09-02%5Bpdf