Cancer GIS studies a powerful and unexploited
technique but convolution must be taken into account and correlation or
anti-correlation doesn’t always mean causation unless you’ve got occupation or
infection then surely you have revelation?
Revised
June 2015 By Dr Chris Barnes, Bangor
Scientific and Educational Consultants
e-mail doctor.barnes@yahoo.co.uk
Homepage
for more cancer and other research http://drchrisbarnes.co.uk
Abstract
GIS techniques have been
used to acquire and contrast data for GSM cell phone penetration, Night Light
(wealth index) and Total Sunshine amounts in correlation with incidence
statistics for 10 common cancers on a global scale. A huge wealth of
information is apparent in the main data table some at first sight
unexpected. A systematic explanation of
the correlated behaviour of each cancer in sign and magnitude is given in terms
what is already known or is beginning to be found out or even hypothesised upon
in the contemporary literature regarding occupational occurrence and/or
causation by disease.
Introduction
One motive behind this
work is to try and get the decision makers of this world to sit up and listen
regarding the absolutely undeniable link between breast cancer and light at night. Despite there being approaching 400
publications in 2015 alone and over 3000 since 2014 typical cancer information
websites such as http://www.cancerresearchuk.org
[1] do not even mention the
link. Instead they prefer to tell us women get breast cancer because they are
too affluent, eat too much fat, have babies at the wrong time or use the Pill
or HRT.
I have already show in a
previous publication the undeniable link between breast cancer and lack of
sunlight (VITAMIN D) [2] and
explained how government propaganda to keep out of the sun and slap on the
sunscreen is exacerbating the situation.
A second motive behind
this publication is to attempt to firm up on the link between various cancers
and RF radiation. I have also published
extensively on this topic elsewhere.
It is easy to see how
links between cancer and affluence might arise. GIS techniques for example have
allowed affluence index to be computed because it mimics the amount of light
shone into space and detectable by satellite.
Also if you are affluent you are more likely to consume a lot of dairy. The more light at night you have the less
melatonin nature’s anti- tumour proliferation and cancer agent. Too much dairy actually leaches the vitamin
D on think at first sight it ought to be supplying. It is clear to see that there are two
mathematically convoluted functions at work here.
A solar index too, could
have double entendre when it comes to its use in predictive cancer aetiology as
it may correlate with vitamin D provision but then again there is often more
sun in the developing world so there will be convoluted correlation with nasty
infections as well. Vitamin D is often
cancer protective, infections fuel cancer so we may therefore expect the signs
as well as magnitudes of these correlations to change according to cancer
type.
Mobile phone penetration
as well as being an indicator of finding places where there will be RF fields
is perhaps also to be an indicator of wealth.
Once again any attempt which attempts to correlate geo-spatial cancer
incidence with this parameter must take into account that the convoluted
factors of wealth and Radio Frequency fields could potentially have opposite
kinds of effects when it comes to cancer aetiology.
Experimental
I have taken incidence
data for world cancers from cancer.org website, global cancer facts and figures
2008 [3]. I have used data for Bladder, Breast, Cervix,
http://www.cancerresearchuk.org
Colorectal, Liver, Lung, NHL, Oesophageal, Prostate and Stomach cancer. I used all sex average data with the
exception of course of the male and female cancers and Lung and Stomach where
female only data was used. I did this
because there are large parts of Russia/ Asia /China where smoking is mainly
done by males and I wanted to explore these cancers in a more general and less
weighted context.
I have taken GSM data
from Vodafone and I have taken light at night wealth index data from ‘The World
at night ‘index[4]
 I
estimated percentage wealth as being equal to 100 - % of population in poverty.
I
estimated percentage wealth as being equal to 100 - % of population in poverty.
Individual graphical
linear correlations were performed
using CurveExpert 1.4 [5] and p-values were calculated from R values and the number of
degrees of freedom for each plot using an online calculator [6].
The data was condensed
into a single XL file.
Results
and Discussion
The results are shown in
Table 1 below:
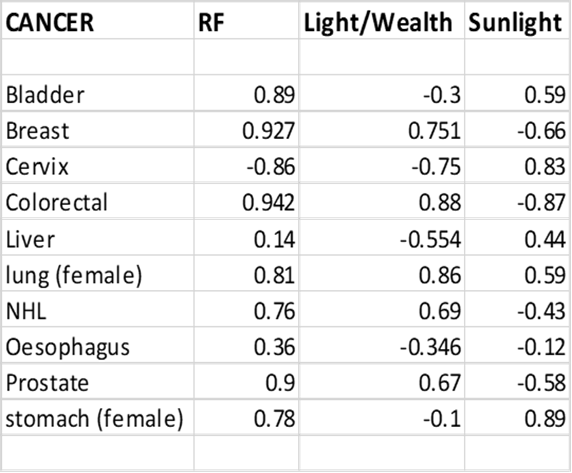
Table
1
The cancers I have
typically described previously as the RF cancers i.e. Breast and Prostate show
virtually identical correlations in this study.
NHL and Colorectal cancer also show a similar trend. These four cancers
would appear to be positively correlated with RF and with Light at Night (both
of which could also be wealth indicators) and negatively correlated with
sunlight i.e. more vitamin D equates with less cancer. Only by data mining the literature on
occupational effects can we expect to glean to true correlation/ causation
here. I will proceed to explore this
facet for every individual cancer in the study later in this present
discussion.
The cancers least
positively correlated with RF appear to be those of the Cervix (which is highly
negatively correlated), Liver and Oesophagus which are not statistically
correlated. Since these are all cancers
known to be associated to a greater or lesser extent with infective agents
likely to be more prevalent in poor areas of the world, an anti-correlation
with wealth ( as in this case measured by night light) is to be expected and is
indeed found. In the case of cancer of
the Cervix GSM penetration appears simply to be acting as a comparable wealth
indicator to night light but with liver cancer and Oesophagus cancer the two ‘wealth indicators’ have correlations, although weak of opposite
sign and worthy of further investigation. In the case of stomach cancer the two
‘wealth indicators are also of opposite sign but the weighting is
reversed. Clearly something very complex
is happening here and I will attempt an explanation when dealing with each
individual cancer.
Discussion
of Individual Cancers
1. Bladder
Bladder cancer appears to
be negatively correlated with Light at Night or more likely wealth index. There is a positive
correlation with sunlight suggesting an excess of incidence in hot/tropical
countries. Mostafa et al (1999) [7] have explained that carcinoma of
the urinary bladder is the most common malignancy in the Middle East and parts
of Africa where schistosomiasis is a widespread problem. Theirs and much other
evidence supports the association between the parasitic infection
schistosomiasis and bladder cancer. Schistosomes are thought to account for about .1% of all
cancers worldwide. This means that given
bladder cancer varies between been about the 6TH and 10th
most common cancer in the world that schistosomes
probably account for between 1-2% of all bladder cancers worldwide. Up to 27% of female bladder cancer may be
associated with recurrent UTI. However,
by far the most bladder cancer is, nevertheless, still thought to be associated
with smoking.
As distinct from the inverse
correlation of bladder cancer in this present study with Light at Night, there
is seen a significant positive correlation with mobile phone penetration (RF
energy).
Interestingly, Törnqvist
et al [8] studied a cohort of 3358 power
linesmen and 6703 power station operators classified in the 1960 population
census in Sweden. The cancer incidence
between 1961 and 1979 was calculated in relation to all male blue collar
workers. The relative risk of cancer (all sites) was 1.1, (1.0-1.2, 90%
confidence limit) in the group of power linesmen and 1.0 (0.9-1.0) for power
station operators consistent excess risk of leukaemia or brain tumour was found
in the two occupational groups. In both groups a tendency towards an excess risk of cancer of the
urinary organs was found.
This is somewhat
supportive of the observed association between bladder cancer and RF in my
present study in so far as both provide electromagnetic fields albeit of
different frequency. The link is most
possibly in the effect of RF fields on melatonin.
For example, the pineal
hormone melatonin has been shown to reduce the incidence of
experimentally-induced breast cancer in rats, the hormone is oncostatic and cytotoxic to breast, ovarian, and bladder
cancer cell lines in vitro [9]. Thus, logically, with a lack of
melatonin, the converse, might be
expected to be true. There is indeed
evidence for RF fields causing such a reduction.
Burch et al 2002 [10]
showed that there are exposure-related reductions in 6-OHMS excretion where
daily cellular telephone use of >25min was more prevalent. Prolonged use of
cellular telephones may lead to reduced melatonin production, and elevated
60-Hz MF exposures may potentiate the effect, combining this with the results
of Zhang above yields elegantly
consistent support with the observed positive regression for stomach cancer and mobile phone
penetration in this present work.
Also Read more at: http://informahealthcare.com/doi/abs/10.1080/09553000210166561
2. Breast
There are more than 500 Papers Published in
2015 so far which mention a link between
breast cancer and the circadian rhythm. There are more than 3000 papers
published in 2014
321 papers in
2015 so far mention Melatonin and some 2500 in 2014.
2900 papers mention Vitamin D in 2015 alone! The most explicitly titled of all these
papers is that of Stevens et al 2009 [11] ‘Breast cancer and circadian disruption from electric lighting in the modern
world’.
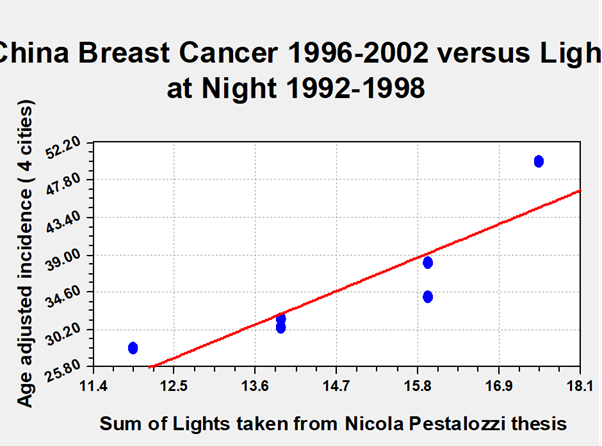
Taking all the above into account, in this case I
believe my result for breast cancer and
nightlight certainly demonstrates the
notion of correlation with causation.
On the basis that night light also indicates wealth,
as could GSM penetration (RF), the inter correlation between the two could of
course yield up a positive correlation for breast cancer irrespective of
whether or not there is actual causation by RF.
In order to be more certain, I shall look for other documented effects
of RF and breast cancer and for occupational effects.
West
el al (2013) [12] report a case of a series of four
young women—ages from 21 to 39—with multifocal invasive breast cancer that
raises the concern of a possible association with non-ionizing radiation of
electromagnetic field exposures from cellular phones. All these women patients
regularly carried their Smartphone’s directly against their breasts in their
brassieres for up to 10 hours a day, for several years, and developed tumours
in areas of their breasts immediately underlying the phones. All patients had
no family history of breast cancer, tested negative for BRCA1 and BRCA2, and
had no other known breast cancer risks. Their breast imaging showed clustering of multiple tumour foci in
the breast directly under the area of phone contact. Pathology of all four
cases shows striking similarity; all the tumours were hormone-positive and of
low-intermediate grade, having an extensive intra-ductal component, and all the
tumours had near identical morphology. These cases raise awareness to the lack
of safety data of prolonged direct contact with cellular phones.
Kliukiene et al 2003 [13] studied occupational exposure to
RF and 50 Hz fields in female radio operators. The exposure was assessed in two age
groups (<50, 50+) with regard to risk of breast cancer. The odds ratios in
the group with the highest cumulative exposure were 1.78 (95% CI 0.59-5.41) and
2.37 (95% CI 0.88-6.36) in the younger and the older women, respectively.
P-value for trend was a statistically very relevant 0.03 in both age groups.
The results of the oestrogen receptor status analysis by exposure to EMF showed
an increased risk of oestrogen receptor-positive breast cancer in the younger
women, while the older age group had an elevated risk of oestrogen
receptor-negative breast cancer. Thus, the present study contributes to the
hypothesis of an association between occupational exposure to EMF and increased
risk of breast cancer. The fact that the tumours were hormone positive in younger women is
exactly in line with the observation of West above.
My results show a significantly higher correlation coefficient for breast cancer incidence with the GIS parameter GSM penetration than with night lighting. Even if part of the effect is cross correlation I am convinced given the detail above that based on this result and taken with several of my other studies that RF radiation in this case specifically GSM cell phone radiation is a significant hazard and presents a significant risk for female breast cancer. The occupational study on radio operators followed some women since the 1960’s. Since mobile phone penetration in any significant numbers only began less than two decades ago it is early days to have completely firm data. Although mobile phones emit lower power than a ship’s transmitter we are in closer bodily proximity to them and often for much longer periods. Thus field strengths could be comparable. Frequency and modulation schemes for causing cancer, which I have also discussed elsewhere [14, 15], could be critical and this explains why some in vitro studies and some animal studies have negative results and others have positive results. Certainly it has, very recently indeed also been shown that a.m. modulated radio waves at very specific frequencies can reverse cancer as can 48 GHz microwaves.
3.
Cervix
The correlations for cancer of the cervix are the exact opposite in sign to those for breast cancer. This I ascribe to a sign that poor socio-economic conditions rather than affluence favours this cancer. Cancer of the cervix is known to be closely associated with HPV infection. HPV is rifer in the developing world where there is often less screening and more promiscuity. Also HPV vaccination is now used in many developed countries which has also stabilised incidence rates. The positive correlation with sunshine is presumably because a lot of the developing world countries are in tropical/equatorial positions with high sunshine totals. Pisani et al (2011) [16] estimated that a massive 89% of all Cervical cancers may be due to human papillomaviruses.
4.
Colorectal
The magnitude and signs of the correlations here are very similar to those observed for breast cancer. Simplistically, colorectal cancer has been associated with junk food style western diets and the three correlations express this. However, as we saw earlier with breast cancer Light at Night is a causative agent as well as affluence. Similarly, lack of sunshine means lack of Vitamin D and breast cancer was thus negatively correlated with sunshine as is colorectal cancer.
In a similar manner then, I will search for and
present evidence of association of colorectal cancer with Light at Night (low
melatonin levels) and low sunshine amounts.
Occupational studies regarding the association between night shift work
and colorectal cancer and chronic disease in general are always the most useful
here. There are indeed vast numbers of example publications but a good general
example is given by Wang et al (2011) [17].
It has also been shown that melatonin, known to be heavily suppressed by light at night as found in more affluent parts of the world, is a potential chemotherapeutic agent for treatment of colon cancer, the effects of which are mediated by regulation of both cell death and senescence in cancerous cells with minimized cardio-toxicity, see Dauchy et al (2102) [18]. Thus once again as with breast cancer I suggest that correlation is indeed in this highly likely to also be causation and the latter by a double edged sword.
5.
Liver
The result for Liver Cancer is similar to that for Cervix cancer in that the sign of the correlations for Night Light (wealth index) and for sunshine are as for Cervical Cancer but the sign of the correlation for GSM (RF) is opposite but is so small as to be not statistically significant.
In any event unlike with breast cancer there is experimental evidence, albeit from an animal model (rat) that RF fields at GSM frequencies do not promote liver cancer.
These findings of K Imaida (
1998) [19] clearly indicated that local body exposure
to a 929.2-MHz field, modulated in a PDC waveform, has no significant effect on
rat liver carcinogenesis under the experimental conditions employed. Furthermore in another study local body exposure to a 1.439
GHz EMF, as in the case of a 929.2 MHz field, had no promoting effect on rat
liver carcinogenesis in the present model.
This adds some weight to the very low observed correlation factor with GSM in my present study and casts doubt on the earlier suggestion that GSM penetration may be as good a wealth index indicator as Light at Night. However, such disparity could occur with any convoluted correlation function.
Pisani et al [16]
estimated that 15.6% (1,450,000 cases) of the worldwide incidence of cancer in
1990 can be attributed to infection with either the hepatitis B and C viruses,
the human papillomaviruses, EBV, human T-cell lymphotrophic
virus I, HIV, the bacterium Helicobacter pylori, schistosomes,
or liver flukes.
Further they indicated the disparity in cancers in
developing countries suggesting that
there would be 21% fewer cases of cancer in developing countries (1,000,000
fewer cases per year) and 9% fewer cases in developed countries (375,000 fewer
cases per year) if these infectious diseases were prevented.
The attributable fraction at the specific sites
varies from 89% of cervix cancers attributable to the papillomaviruses to 1% of
all leukemias attributable to human T-cell lymphotrophic virus.
My present work suggests that
when cancer is negatively correlated with Light at Night or wealth index,
significant infective agents are at play. Perz et al (2006) [20]
found that HBV and HCV infections
account for the majority of primary liver cancer (78%) throughout most of the
world, highlighting the need for programs to prevent new infections and provide
medical management and treatment for those already infected.
6.
Lung
The result for female lung cancer appears strange at first sight. This cancer appears to be positively
correlated with all the factors in the investigation. I will endeavour to explain this by extensive
data mining of the existing literature.
A study of Lissoni et al (2003) [21] was performed to assess the 5-year survival
results in metastatic non-small cell lung cancer patients obtained with a
chemotherapeutic regimen consisting of cisplatin and etoposide, with or without
the concomitant administration of melatonin (20 mg/day orally in the
evening). The study included 100 consecutive patients who were randomized to
receive chemotherapy alone or chemotherapy and melatonin. Both the overall tumor regression rate and the 5-year survival results were
significantly higher in patients concomitantly treated with melatonin. In
particular, no patient treated with chemotherapy alone was alive after
2 years, whereas a 5-year survival was achieved in three of 49 (6%)
patients treated with chemotherapy and melatonin. Moreover, chemotherapy was
better tolerated in patients treated with melatonin. This study confirms, in a
considerable number of patients and for a long follow-up period, the
possibility to improve the efficacy of chemotherapy in terms of both survival
and quality of life by a concomitant administration of melatonin. This suggests
a new biochemotherapeutic strategy in the treatment
of human neoplasms.
It is thus my hypothesis that melatonin may well also be protective against lung cancer in the absence of chemotherapy or in healthy individuals, hence the observed positive correlation of this cancer with Light at night, a known suppressor of melatonin. Another known possibility is that more women smoke in more affluent countries, see Amos (1996) [22]. There are thus major dichotomies between the distribution of male and female lung cancer worldwide.
Cheng et al (2001) [23] has shown a very strong association of Human Papillomavirus 16/18 Infection with Lung Cancer among Non-smoking Taiwanese Women. Only 10% of Taiwanese women smoke and the odds ratio for lung cancer is over 10 with these types of HPV infection.
Kirk et al (2007) [24] has also shown HIV Infection Is Associated with an Increased
Risk for Lung Cancer, Independent of Smoking.
Chlamydia pneumoniae infection associated with
chronic bronchitis has also been associated with lung cancer in smokers and in
passive smokers, see these examples but not exclusively, Kocazeybek
(2003) [25] and Laurila
et al (1997) [26] and Littman et al
(2005) [27].
So above are considered three infections which can
significantly influence lung cancer statistics.
Infections are often more prevalent in hot tropical countries, thus this
probably explains the observed positive correlation with sunshine.
Clearly, the melatonin effect is overwhelming the
tendency for lung cancer to correlate with poverty hence the unusual and perhaps unexpected
positive correlation with light at night (wealth index).
There is no suggestion in the literature that Lung
Cancer is in any way correlated with RF radiation so that the positive correlation with GSM (RF) penetration is
either a new observation or because it is cross correlated with light at night. If this is a new observation it may be
suggestive that RF in this case is simply a melatonin inhibitor. There are numerous anecdotal reports of people either finding it difficult to
sleep or getting sleep disturbances near mobile phone base stations. There are
also references too numerous to mention which refer to the effect of RF and EMF
on the pineal gland.
7.
NHL
I have previously identified NHL as an RF sensitive cancer
along with breast and prostate, see http://www.drchrisbarnes.co.uk/World.htm
[28].
In this present work, the result for NHL is observed to follow the same fundamental pattern as for breast cancer.
Drake et al (2010) [29] have shown that low serum vitamin D levels lead to poorer EFS (event free survival) in T-cell lymphoma.
This is highly consistent with the negative
correlation of NHL cancer with sunlight amounts observed here.
Occupational
studies on night shift work showed that the risk of NHL is increased albeit
only by a small factor 1.1, see Lahti et al (2008) [30].
This and my present result suggest a melatonin
involvement with NHL. Evidence in support of this notion comes from the fact
that Todisco (2007) [31] has successfully treated a case of
Low-grade Non-Hodgkin Lymphoma at Advanced Stage with Cyclophosphamide Plus Somatostatin,
Bromocriptine, Retinoids, and Melatonin.
Light at Night destroys melatonin and the
observation here of positively
correlated NHL incidence with this factor is thus to be expected.
A study of US Radio Ham
operators was carried out in order to assess possible effects of
electromagnetic fields on human health.
The all-cause standardized mortality ratio (SMR) was 71, but a
statistically significant increased mortality was seen for cancers of the other
lymphatic tissues (SMR = 162), a rubric which includes multiple myeloma and
non-Hodgkin's lymphomas, see Milham Jr. (1988) [32].
This is consistent with
the observation of a positive
correlation of NHL incidence with GSM penetration.
The mechanism here is
unclear. It could be a similar
interference of RF with melatonin levels as that proposed for Lung Cancer.
8.
Oesophagus
The result for Oesophagus
cancer appears to be unique in that it appears to be the least correlated of any of the cancers considered.
Furthermore, there is a weak positive correlation against GSM (RF) and weak
negative correlations against Night at Light and Sunshine.
A negative correlation
against Light at Night has been shown here be more expressly a negative
correction with Wealth index and therefore indicative of a cancer associated
with infection. The has been confirmed for several of the other cancers
considered and so we may, perhaps, expect something similar in the case of
oesophageal cancer. I have searched for
such associations with success.
For instance, Syrjänen
et al (2002) [33] have shown that
infection with the human papillomavirus (HPV), notably HPV type 16, has been
associated with oesophageal cancer in seroepidemiological
studies. Interestingly this association seems to be consistent in many
different countries of the world.
A negative correlation
with sunlight suggests that good vitamin D status may be protective against
Oesophagus cancer. Giovannucci et
al (2006) [34] has shown that low levels of vitamin D may be associated with
increased cancer incidence and mortality in men, particularly for
digestive-system cancers. This gives us
a strong pointer that with Oesophagus cancer correlation and causation in this
present study do go hand in hand.
There would appear to be
nothing in the present literature linking Oesophagus cancer to RF radiation.
The Oesophagus is deep inside the body and the penetration depth of GSM and
WIFI is probably too small to influence it.
In any event a regression factor
of .36 is rather small.
9.
Prostate
Cancer
I have previously
identified prostate cancer as an RF sensitive cancer, see Barnes [35].
The results of this present GIS study confirm the same. Prostate cancer is also positively correlated
with Light at Night and negatively correlated with Sunshine. There are numerous references to the
protective aspects of both vitamin D and Melatonin in prostate cancer.
For
instance, Schwartz
and Hulka (1990) [36] indicate that prostate cancer is a major cause of cancer death
among males, yet little is known about its aetiology. They hypothesize that
Vitamin (Hormone) D deficiency may underlie the major risks for prostate
cancer, including age, Black race, and northern latitudes. The factors they
mention are all are associated with decreased synthesis of Vitamin D. Further
they observe that mortality rates from prostate cancer in the U.S. are
inversely correlated with ultraviolet radiation, the principal source of
Vitamin D. This hypothesis is consistent with known antitumor properties of
Vitamin D, and may suggest new avenues for research in prostate cancer. Their work gives considerable support to my
present study. Viewed in conjunction with other recent data, including those
demonstrating a differentiating effect of vitamin D on human prostate cancer
cells, these and my present findings
suggest that vitamin D may have an important role in the natural history of
prostate cancer.
The
results of Moretti et al ( 2000) [37] indicate that melatonin, at nanomolar concentrations, exerts a direct antiproliferative
action on androgen-dependent prostate cancer cells, significantly affecting
their distribution throughout the cell cycle.
Again in strong support of the notion that the correlations
I observe for prostate cancer are
causative.
10.
Stomach Cancer
The result for stomach cancer can be interpreted as
follows. The negative correlation with
night light index is more than likely a wealth factor and therefore indicative
of cancer whose incidence is controlled primarily by infection. The negative correlation is, however, weak
and my interpretation is that it may be being partly offset because of a
melatonin effect. The strong positive
correlation with sunshine is suggestive of a cancer prevalent in developing
countries.
With regard to infection, Uemura,et
al (2001) [38] showed that gastric cancer develops in
persons infected with H. pylori but not in uninfected persons.
Bardhan
(1997) [39] has showed that
Helicobacter pylori
infection has a worldwide distribution, and it has distinct epidemiological
features in developing countries. These are of course usually the sunnier
countries of the world which is consistent with my observations. In contrast to that in developed countries, H.
pylori infection in developing countries seems to be nearly universal,
beginning in early childhood. Children become infected in the first few months
of life; in some communities as many as 50% of the children are infected by the
age of 5 years, and up to 90% are infected by the time they reach
adulthood. This is again exactly consistent with my present observations and showing the GIS
technique developed here to be incredibly powerful.
There are no significant references to correlations
of RF radiation with stomach cancer. Mobile phone penetration in Africa is an
alternative to wealth index as derived from NLDI (night light development
index). NLDI is negatively correlated
with a very high correlation factor approaching .9, whereas GSM is only correlated
at .66. Nevertheless, the result for
gastric cancer may well be revealing something new. However, I would expect a negative correlation rather
than a positive correlation if RF were not involved at all. Perhaps if RF is involved, it is in that it
is more effective in reducing melatonin than light at night or perhaps there is
another as yet undisclosed mechanism.
The results of Zhang et al (2013)
[40], showed that melatonin
could inhibit cell proliferation, colony formation and migration efficiency,
and it promoted apoptosis of SGC7901 cells. Their findings suggest that the
anti-cancer effects of melatonin may be due to both inhibition of tumour cell
proliferation and reduction of the metastatic potential of tumour cells. This is consistent with my hypothesis for the weakening of the wealth index
correlation effect in favour of melatonin as described above.
Burch et al (2002) [41]
showed that there are exposure-related reductions in 6-OHMS excretion
where daily cellular telephone use of >25min was more prevalent. Prolonged
use of cellular telephones may lead to reduced melatonin production, and
elevated 60-Hz MF exposures may potentiate the effect, combining this with the
results of Zhang above yields elegantly
consistent support with the observed positive regression for stomach cancer and mobile phone
penetration in this present work.
Read More: http://informahealthcare.com/doi/abs/10.1080/09553000210166561
Conclusions
In this comprehensive and worldwide GIS based study of 10 common cancer
types it has been possible to fully account for their individual aetiology from
a comparison of the regression coefficients of their incidence versus the three
potential but convoluted correlating functions considered.
Ready known facts concerning the aetiology of disease associated cancers
particularly in the third world are supported /confirmed and a new dimension is added to cancer
aetiology of the developed world.
Evidence is raised to suggest that RF emissions from cell phones may be far
more relevant to a larger number of cancers than previously thought and if this
is so general mechanisms such as melatonin suppression and/or oxidative stress
are the most likely.
Because the correlating
functions are in themselves convolutions and can never be anything else then
where infectious disease is the major cause of cancer it can even reverse or
vastly reduce the correlation coefficient for the RF effect.
For example take cervical
cancer known to have its causes rooted in 89% disease and yielding a regression
factor against GSM penetration of
-.86 and Liver cancer which has some 15%
of its occurrence related to disease yielding R(GSM)=.14. 11% of oesophageal
cancer may be due to infection R GSM =.36.
Any wealth index correlates well in a negative sense with disease.
Both GSM and Night Light
(Wealth) are approximately anti-correlated with the percentage of any cancer
whose causes are rooted infection. The
effect of driving the numeric value of the regression factor farthest negative
is, however, is more pronounced for a wealth index based on night light then on
mobile phone penetration. This might
simply be because Night Light Index is a better correlator of wealth/poverty in
the first instance and/ or alternatively/ it could be because RF (radio
frequency) technologies such as GSM are even more effective at suppressing
melatonin/ promoting cancer than Light at Night.
This phenomenon can be
explored further by plotting directly the GSM correlation coefficients against
the Light at Night regression. When this is done the result is a remarkably
good linear correlation.
This is suggestive that
GSM is far more active in its propensity to drive cancer than is Light at
Night.
Perhaps the world needs
to sit up and listen?
References
1.
http://www.cancerresearchuk.org
2.
http://www.drchrisbarnes.co.uk/blbr.htm
4.
http://www.worldatnight.ethz.ch/index.php?chapter=home§ion=references.
5.
http://www.curveexpert.net/curveexpert-basic/
6.
http://graphpad.com/quickcalcs/PValue1.cfm
7.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC88908/
8.
http://oem.bmj.com/content/43/3/212.abstract
9.
http://www.ncbi.nlm.nih.gov/pubmed/8061240
10. http://www.ncbi.nlm.nih.gov/pubmed/12456290
11. http://www.sciencedirect.com/science/article/pii/S138357180900271X
12. http://www.hindawi.com/journals/crim/2013/354682/
13. http://www.ncbi.nlm.nih.gov/pubmed/12883383
14. http://www.drchrisbarnes.co.uk/RFAS.htm
15. http://www.drchrisbarnes.co.uk/Space.htm
16. http://www.ehjournal.net/content/10/S1/S2
17. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3045028/
18. http://cancerres.aacrjournals.org/content/72/8_Supplement/165.short
19. http://carcin.oxfordjournals.org/content/19/2/311.full.pdf
21. http://www.ncbi.nlm.nih.gov/pubmed/12823608
22. http://bmb.oxfordjournals.org/content/52/1/74.abstract
24. http://cid.oxfordjournals.org/content/45/1/103.full
25. Kocazeybek
http://jmm.sgmjournals.org/content/52/8/721.full
26. http://www.ncbi.nlm.nih.gov/pubmed/9036866
27. http://cebp.aacrjournals.org/content/14/4/773.full.html
28. http://www.drchrisbarnes.co.uk/World.htm
29. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2953973/
30. http://onlinelibrary.wiley.com/doi/10.1002/ijc.23566/full
32. http://www.ncbi.nlm.nih.gov/pubmed/3422125
33. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1769774/
34. http://www.ncbi.nlm.nih.gov/pubmed/16595781
35. http://drchrisbarnes.co.uk/TVCAN.htm
36. http://www.ncbi.nlm.nih.gov/pubmed/2241107
37. http://www.ncbi.nlm.nih.gov/pubmed/10671684
38. http://www.ncbi.nlm.nih.gov/pubmed/11556297
39. http://www.ncbi.nlm.nih.gov/pubmed/9402340
40. http://www.ncbi.nlm.nih.gov/pubmed/23477595
41. http://www.ncbi.nlm.nih.gov/pubmed/12456290
42.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|