Dotting the I’s and crossing the T’s on the mechanism of the 27 MHZ AM ‘Therabionic’ low power cancer treatment system, an independent theoretical assessment by Dr C.Barnes, manager BSEC-WALES. 17th November 2022.
Abstract
The Therabionic cancer therapy system is discussed and summarised. Historic ideas for its mechanism are discussed. In summary these were In summary the conclusions were that
1. The Therabionic system could be interfering with multiple ion or amino acid transporters but that to additionally account for the pulse and blood pressure/nervous system interactions there would have to be involvement of Ca2+ channels of which of which L,T and N types exist.
2. When taking bio-soliton approach to the problem , the 2,221.323 Hz is the easiest frequency to relate to (1) above.
3. Based on a purely theoretical approach to the then science of cancer biology, chemical knockdown agents and voltage gated channels, it was then concluded that CA2+ efflux or slowing of influx was involved. This is the direct opposite of the conclusion recently reached by Jimenez.
The recent findings of Jimenez concerning the involvement of the membrane CAV3.2 channel in hcc stem cell pathology is highlighted. The likely conclusions of the Jimenez these are thus
1. RF AM EMF has anti-proliferative action in HCC carcinoma stem cells via the T-type CAV3.2 channel.
2. It is likely this channel is involved in the TTF identification via changed pulse rate as well.
3. The physical mechanisms of the RF interaction remain undisclosed.
4. The reasons why there are multiple TTF frequencies at very high harmonic values of possible ICR frequencies also remain undisclosed.
Thus, at such stage true mechanisms of AM modulated RF energy on the channel and the reasons for pulse and blood pressure changes remain unknown. As do the reasons for large numbers of TTF frequencies and their very high Q values.
The present paper thus goes on to discuss the therabionic technology from its origin as a sleep aid to its present position as a cancer treatment device. It is supportive of Jimenez findings but by developing a new theory of channelopathy and RF interaction it takes these to the next level. CaV3.2 involvement is present but other channels cannot and must not be overlooked. Demodulation effects in channels is explained and findings similar to those of therabionic are reported experimentally for plant biological systems. Not unreasonable due to the ubiquitous nature of voltage gated ions channels and transporters throughout the eukaryotic world. The paper provides theoretical and experimental grounds for the highly frequency selective demodulation process in ion channels as a real process and given the induced jumps in voltage above could well be one that gives rise to changed pulse rate and/or blood pressure in the patients in the Therabionic cancer study. Dangers of off target effects with channels blockers and anti-cancer drugs are also raised as is the involvement of the endoplasmic reticulum in hcc cancer. I conclude that the involvement of TTF’s with CAV3.2 influx as cited by Jimenez is a real effect in both the TFF determination itself through pulse/blood pressure changes and the anti-cancer activity. However, based on my theoretical analysis I cannot conclude it is the only anti-cancer effect at work. Further the mechanism of the pulse/blood pressure effect, CAV3.2 and many other families of voltage gated ion channels and transporters are ubiquitous in excitable tissue. In order for the patients to feel a ‘jolt’ in pulse change when the TTF modulation frequency is appropriately ‘tuned’ there must be a coincident change in nerve action potentials. I have no reason to suppose that CAV3.2 could not bring about such a change but neither do I have a reason to suppose that other voltage gated channels would not be able to achieve the same or similar. In other words, not every frequency that is listed as a TTF may be a frequency that changes ion flow in CAV3.2 either in excitable or non-excitable tissue. Although strongly supported, the dehydrated ICR hypothesis will only be fully confirmed when the groups concerned decide to make an exploration of TTF frequency change versus GMF field change.
Introduction
The TheraBionic P1 produces low levels radiofrequency (RF) electromagnetic fields at 27.12 MHz , which are amplitude-modulated at tumor-specific frequencies. The device is coupled with a spoon-shaped antenna, which is placed in the patient’s mouth, more precisely on the anterior part of the patient’s tongue for three sixty-minute sessions per day. When the spoon-shaped antenna is placed on the patient’s tongue, it delivers low levels of radiofrequency electromagnetic fields throughout the patient’s body.
Tumour shrinkage as assessed by radiological imaging as well as changes in AFP levels were documented in patients with advanced HCC receiving RF EMF modulated at HCC-specific frequencies administered by the intrabuccal probe. Antitumor activity in patients with advanced HCC was exemplified by partial responses observed in four patients (9.8%) and decreases in AFP levels greater than 20% in four patients. A total of 18 patients (43.9%) either had objective response or SD for greater than 6 months. Importantly, clinical benefit also was observed in patients with Child Pugh B disease, i.e., patients with severely impaired liver function who tolerate poorly antitumor treatment with drugs such as sorafenib (Nexavar®), Lenvatinib (Lenvima®) or regorafenib (Stivarga®).
Of the 41 patients in the initial clinical trail , 14 patients (34.1%) had stable disease (SD) for more than 6 months, which met the pre-planned primary efficacy criterion of 8 patients with progression-free survival of at least 6 months. Median progression-free survival was 4.4 months (95% CI 2.1–5.3) and median OS was 6.7 months (95% CI 3.0–10.2). Estimated survival at 12, 24 and 36 months was 27.9% (s.e. = 7.1%), 15.2% (s.e. = 5.7%), and 10.1% (s.e. = 4.8%), respectively. Overall, there were six long-term survivors with an OS greater than 24 months and four long-term survivors with an OS greater than 3 years. Importantly, five of the six (83%) long-term survivors had radiological evidence of disease progression at the time of study enrolment. Two of three patients with the longest survival (44.6 and +58 months) had radiological evidence of disease progression at the time of enrolment, and BLCL stage C disease. The latter patient remained on therapy with a near complete response for 58 months.
In 2001 Pasche and Barbault began examining patients with a diagnosis of cancer with the goal of identifying cancer specific frequencies. Using non-invasive devices at both 433 MHz and 27.12 MHz emitting very low and safe levels ( INCRPP) ( SARs ranging from 0.02 mW/kg to 400 mW/kg)of radiofrequency electromagnetic fields, commonly named radio waves, they discovered that patients with a diagnosis of cancer exhibited subtle but reproducible changes in their palpable pulse and blood pressure when exposed to certain AM modulation frequencies. Next, they hypothesized that the frequencies they had discovered could be used to treat cancer and designed a study in which patients were offered treatment with tumor-specific frequencies. Radio waves modulated at these tumor-specific frequencies were delivered for three hours daily by means of a battery-operated portable device connected to a spoon-shaped antenna placed on the patient’s tongue, which results into the delivery of radio waves throughout the body. (Barbault, Costa et al. 2009)
Several patients enrolled in this study, published in 2009, had evidence of either tumor shrinkage or stabilization of the growth of the tumor, confirming the hypothesis that radio waves modulated at specific tumor frequencies could block cancer growth.(Barbault, Costa et al. 2009) This hypothesis was further confirmed in a subsequent study conducted by Costa and collaborators in patients suffering from advanced hepatocellular carcinoma, which was published in 2011.(Costa, de Oliveira et al. 2011) In that study, treatment with the cancer-specific radio waves again resulted in either tumor shrinkage or tumor growth arrest in approximately half of the patients treated.(Costa, de Oliveira et al. 2011)
In 2012, Zimmerman and collaborators working in Pasche’s laboratory demonstrated that the cancer-specific radio waves identified in patients with a diagnosis of cancer were able to block or slow down the growth of cancer cells. These experiments were conducted with laboratory equipment replicating the same radiofrequency levels as those generated in patients receiving treatment with the portable device connected to the spoon-shaped antenna. These experiments also showed that the growth of cancer cells was only blocked when tumor-specific radio waves were used, i.e. HCC-specific radio waves blocked the growth of HCC cells but did not affect the growth of breast cancer cells. Similarly, breast cancer-specific radio waves blocked the growth of breast cancer cells but did not affect the growth of HCC cells. Additionally, radio waves chosen at random did not affect the growth of any cancer cells thus confirming the well accepted concept that randomly-chosen radio waves such as those generated by devices such as cellular phones do not affect the growth of cancer cells or normal cells.
Thus effectively at 2012, the ‘Therabionic’ was a system that had been shown to work but with no known plausible physical mechanism for the interaction of the modulated radio wave and moreover the observed downregulation of two specific genes XCL2 and PLP2 also remained unexplained.
The work came to the attention of BSEC when it fell into the public domain and the scientific literature. BSEC was already hypothesizing on the interaction of radio waves and biological systems in general and had identified and re-evaluated a number of epidemiological studies on the effects of TV and radio transmitters (refs) . Moreover BSEC had evaluated and extended the theory of Geesink and Meijner ( ref). In 2018 BSEC released several papers into the public domain via the website of its manager Dr Chris Barnes. One such paper attempted to explain the above genetic changes and concluded the possibility that a significant number of voltage gated ion channels and /or amino acid transporter channels could be potentially being disturbed, http://drchrisbarnes.co.uk/ct4.htm. Specific conclusions based on ion channel knockdowns by chemical and chemotherapy agents are notoriously difficult to make because many drugs can act both on and off target and trigger changes in the endoplasmic reticulum in addition to the cell membrane. Regarding the specific channels involved another paper ‘Bringing it all together – a brand new explanation of the experimental observations of frequency and power windowing in electromagnetic interaction with biology Hz- GHz, effects of modulations, wound healing, cancer induction/promotion and subtle field cancer treatment’ By Dr Chris Barnes, Manager @bsec-wales.co.uk’ also dealt in a sub-section with the ‘Therabionic’ tumour treating frequencies. The paper also attempted to explain their ‘unusual’ method of bio-feedback selection and further how it helps me narrow the families of ion channels involved. Over-expression of various voltage gated channels in cancer cells is well known. A feature of cancer cells is that the channels often expressed are those normally found in contractile muscle or neural tissue and so I propose to look at the common channels in heart muscle and sensory neurones since firstly, RF perturbation of these is the only way I see the bio-feedback signal could be generated and secondly when such a signal is generated I would then expect the same channels in the patient’s cancer cells to be also modulated. The logic in looking at sensory neurones in addition to heart muscle is just in case the effect was generated in sensory neurones adjacent to the heart or neurones elsewhere mapped to the heart. It discussed C2+ channels and noted that all three types of calcium channel, L,T and N exist in sensory neurones, see Nowycky et al ( 1985). It also noted that in some cases, these Ca2+ channels or pumps are potential therapeutic targets for specific cancer subtypes or correlate with prognosis, see Monteith et al (2012). It showed that 2,221.323 Hz TTF reduces to 277.63 Hz, very close to the 278.9 Hz Geesink condensate/Ca2+ and Cl- (aq) IPR coherence.
It further showed that the only other two most relevant tumour treating frequencies were 10,454.4 Hz TTF thought to be associated with Potassium channels and the 6530.24 HZ TTF
Which reduces to the 408.14 Hz Geesink condensate close to but not directly on either a harmonic of hydronium ion or anhydrous chloride. In this latter respect Hv1 expression is increased in colorectal tumour tissues and cell lines, associated with poor prognosis, see Wang et al (2013). The voltage-gated proton channel Hv1 also plays important roles in proton extrusion and tumour formation by highly metastatic breast cancer cells, see Hong (2014). Thus RF modulation of Hv1 may be critical drug free method in controlling tumour progression and again entirely consistent with the Barnes model.
Peretti et al (2014) have recently disclosed chloride intracellular ionic channels (CLICs) are involved in cancer development. For instance:
•CLIC1 and CLIC4 in particular are overexpressed in cancer stem cells.
•Both proteins are largely present in the cytoplasm of tumorigenic cells.
•In cancer stem cells, they have a functional expression as membrane ionic channels.
•This peculiar localization may offer a unique target for cancer therapy.
More recently, CLC, CLIC, and CLCA intracellular chloride channels have been recognized for their contributions in modifying cell cycle, apoptosis, cell adhesion, and cell motility.
It is emphasised that the above conclusions were purely theoretical. BSEC has no medical or laboratory facilities to evaluate real patient, animal or even cell culture situations.
In summary the conclusions were that
The Therabionic system could be interfering with multiple ion or amino acid transporters but that to additionally account for the pulse and blood pressure/nervous system interactions there would have to be involvement of Ca2+ channels of which of which L,T and N types exist.
When taking bio-soliton approach to the problem , the 2,221.323 Hz is the easiest frequency to relate to (1) above.
Based on a purely theoretical approach to the then science of cancer biology, chemical knockdown agents and voltage gated channels, it was then concluded that CA2+ efflux or slowing of influx was involved. This is the direct opposite of the conclusion recently reached by Jimenez.
We now know that voltage gate ion channels are ubiquitous in the cell. They are not just in the plasma membrane and mitochondrial membrane, but are also found in the endoplasmic reticulum. For example: The endoplasmic reticulum (ER) Ca2+ sensor STIM1, best-known for its essential role in triggering influx of extracellular Ca2+ via Ca2+-release-activated channels when ER stores become depleted, unexpectedly also regulates Ca2+ entry through voltage-gated Ca2+ channels. In response to a drop in ER luminal Ca2+ level, this ER membrane-spanning sensor can contact voltage-gated Ca2+ channels in the plasma membrane and thereby inhibit Ca2+ influx through them. This previously unappreciated, interaction between ER Ca2+ level and magnitude of Ca2+ influx via voltage-gated Ca2+ channels may turn out to powerfully impact Ca2+ signalling in excitable cells, including neurotransmitter release, structural and functional postsynaptic plasticity, and transcription factor translocation. See Sather and Dittmer ( 2019). In HCC, the deregulation of the Ca2+ transportome contributes to tumorigenesis, the formation of metastasizing cells, and evasion of cell death. In this review, we reflect on these aspects by summarizing the current knowledge of the Ca2+ transportome and overviewing its composition in the plasma membrane, endoplasmic reticulum, and the mitochondria, see Lai et al (2022). There are thus strong possibilities for off target action of both channel blockers and chemotherapy drugs. Such cases can potentially allow wildly diametric conclusions to be reached. It is documented for example that in Prostate cancer CAV 3.2 knockdown decreases proliferation. Whereas the opposite is true in colon cancer because increase of cytosolic Ca2+ causes p38 MAPK phosphorylation of p53. Since the RAF/RAS/MAPK pathway is pivotal in cancer progression, I see no reason why the TTF frequencies of Therabionic should only affect CAV3.2 and they could equally be changing the whole transporttome as with any cancer therapeutic drug.
Whilst preparing this work, BSEC contacted the groups involved and discussed ideas with them. At no time was BSEC aware that further research into the Therabionic system was taking place at the Wake Forest Baptist Medical Center: Winston-Salem, NC, US. It came as a recent surprise therefore to stumble on the work of Hugo Jimenez at the aforesaid centre.
In his thesis, Jimenez cites the work of Buckner et al. concluded that specific EMF patterns can affect biological systems by allowing for increased cytoplasmic Ca2+ which then impacts the cell cycle by
changes in cyclin expression. This provides a potential anti-cancer therapy that acts through the T-type VGCC to allow inappropriate influx of Ca2+ resulting in proliferative inhibition. He goes on to discuss
enhanced Ca2+ flux has been shown to be affected by RF exposure in research that dates as far back as the 1970s and in a modulation specific fashion. I would point out here that these early experiments all discuss Calcium efflux situations rather than influx.
Jiminez further states that they sought to identify how Ca2+ enters the cells. Ca2+ entry is mainly controlled by voltage- gated Ca2+ channels (VGCC), which are overexpressed in several forms of
cancer and are implicated in limitless replicative potential, invasion, and metastasis. In doing so, he employed ethosuximide, which blocks all three isoforms (Cav 3.1, 3.2, 3.3) of T-type VGCCs.
Thus, he identified that T-type VGCCs are the necessary mediators of HCC-specific AM RF EMF. Further he states that knockdown of the Cav3.2 isoform did abrogate HCC-specific AM RF EMF’s . Unfortunately, he does not specify whether chemical or gene silencing knock down was employed so it is impossible to tell if ‘off-target’ effects were also present.
Nevertheless. a very significant conclusion was reached since T-type channels operate at the lowest voltages and lowest ionic concentrations of all known channels. Jimenez further explains that the targeted effect of HCC-specific AM RF EMF compared to randomly chosen AM RF EMF is illustrated by tumour reduction and changes in tumour Ki67, cyclin D1, and p21 while the proliferation of intestinal cells and complete blood counts are unaffected. Further his findings establish that tumour reduction mediated by HCC-specific AM RF EMF results from differentiation of HCC into quiescent myofibroblasts. The transformation of HCC into quiescent myofibroblasts contrasts with the well documented association between the EMT phenotype and aggressive HCC32 and adds credulity to this new treatment for hepatocellular carcinoma. He further states that there is a strong rationale for clinical studies combining HCC-specific AM RF EMF with either multi-kinase inhibitors or immune oncology therapies. Certainly, p38MAPK can have a pivotal but often conflicting role in cancer cells and therapies.
It has previously reported that variation in pulse amplitude constitutes the primary method for identification of tumour-specific modulation Frequencies in the Therabionic system which have subsequently been shown to target cancer cell proliferation in a tumour and tissue-specific fashion. Cav3.2 T-type VGCCs are expressed in both endothelial cells and vascular smooth muscle cells of small
arteries, which in turn directly affect pulse amplitude.34 Hence, Cav3.2 T-type VGCCs are thus the most probable link between the vascular system, crucial to the tumour-specific frequency identification process7 and the anticancer effects. However, it should be borne in mind from the extensive work at BSEC that not all the TTF’s are Ca2+ ICR harmonic related.
In cancer a possible functional role of these channels is in mediation of Ca2+ influx that may contribute to Ca2+ oscillations within carcinoma stem cells – these have been observed to occur in the G(1) to S cell cycle transition and with involvement of the endoplasmic reticulum https://www.nature.com/articles/s41419-019-1613-2.
Blocking of the T-type channel did not affect HCC cell proliferation and appears to protect against the antiproliferative effects of AM RF EMF though a mechanism that is yet unknown. The blockade is counterintuitive given the preliminary success of some T-type channel blockers in reducing proliferation and enhancing survival in several cancer types and also discussed previously by BSEC. This suggests that the nature of T-type channel is especially complex, potentially extending to orchestration of intracellular (ER) events either in tandem with, or independently from voltage-
dependent calcium influx. The effect of AM RF EMF acting in concert with these channels may be to perturb Ca2+ oscillations, disrupt intracellular Ca2+levels, the G(1) to S transition, and promote transformation to a quiescent myofibroblast.
Finally, Jimenez states that what remains to be established is the site(s) where the HCC-specific AM RF EMF signal is demodulated so as to influence the changes in pulse pressure
identified in patients with specific cancers7 and the mechanism(s) by which the HCC-specific AM RF EMF signal influences the Cav 3.2 T-type VGCCs on tumour cells. Knowledge of the mechanism(s) should also lead to a better understanding of the precision and effectiveness of the HCC-specific frequencies.
The likely conclusions of the Jimenez these are thus
RF AM EMF has anti-proliferative action in HCC carcinoma stem cells via the T-type CAV3.2 channel.
It is likely this channel is involved in the TTF identification via changed pulse rate as well.
The physical mechanisms of the RF interaction remain undisclosed.
The reasons why there are multiple TTF frequencies at very high harmonic values of possible ICR frequencies also remain undisclosed.
Findings 1 and 2 are not entirely inconsistent with the earlier theoretical proposals of BSEC.
Shortcomings of the Jimenez thesis.
The thesis talks, in its literature review, extensively about ICR/IPR and low frequency Calcium efflux effects. It then goes on to talk about TTF frequencies as though they are somehow related even though they are tens to hundreds of times higher and according to the cancer Biology findings advanced by Jimenez cause Ca2+ influx rather than efflux. Also, there is no explanation of why there is such a large family of TTF modulation frequencies and why they differ for different cancers and even different patients. There is no explanation of AM demodulation by the cell membranes or ion channel(s) involved.
I will endeavour to discuss and elucidate the above.
Reason for the large number of TTF
It is very interesting to note and perhaps somewhat surprising that Jimenez makes no mention of the work of Pasche in 1996, namely ‘Effects of Low Energy Emission Therapy
in Chronic Psychophysiological Insomnia’ Sleep, 19(4):327-336. (1996). Especially given that the 27 MHz AM device employed in that study was essentially the same device as used by Therabionic yet tuned to different and lower modulation frequencies. And indeed, Pasche comments on these frequencies in the first cancer paper, wherein he states that: 42.7 Hz, has a sleep-inducing effect in healthy subjects[25],[26]. However, administration of the same signal to patients with insomnia did not yield any therapeutic benefits. In contrast, administration of a combination of the four frequencies most commonly identified in patients with chronic insomnia (2.7 Hz, 21.9 Hz, 42.7 Hz, and 48.9 Hz). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3845545/
The original patent for the Therabionic system is to be found at http://www.rexresearch.com/pasche/pasche.htm covering TTF frequencies for several different types of cancers ranging from as low as 78 Hz up to some 60 KHz, with the vast majority of frequencies lying between about 1-12 KHz.
Other than the very lowest cancer treating TTF which appears to be of the order of 78Hz all the remaining frequencies are very different.
It is however, perhaps, first worthwhile enquiring if the lower frequencies, say in the sleep study can be associated with ICR and ion efflux of any sort as described for EMF’s in general in the literature study. Yoshida et al https://www.pnas.org/doi/abs/10.1073/pnas.1806486115 address molecular mechanisms regulating sleep duration, a simple computational model of a cortical neuron [simplified averaged neuron (SAN) model], which recapitulates the electrophysiological characteristics of slow-wave sleep (SWS) and wakefulness. They show that comprehensive bifurcation and detailed mathematical analyses predicted that leak K+ channels play a role in generating the cortical electrophysiological characteristics of SWS, leading to a hypothesis that leak K+ channels play a role in the regulation of sleep duration. They comprehensively generated and analyzed 14 knockout mice of the leak K+ channel family, which demonstrated that impairment of the leak K+ channel (Kcnk9) decreases sleep duration. Their results confirmed the validity of the SAN model and suggest a molecular mechanism regulating sleep duration.
Further Tatsuki et al (2016) https://www.frontiersin.org/articles/10.3389/neuro.02.013.2009/full also reported on the detailed molecular mechanisms underlying the regulation of sleep duration in mammals, stated as still being elusive. To address this challenge, they constructed a simple computational model, which recapitulated the electrophysiological characteristics of the slow-wave sleep and awake states. Comprehensive bifurcation analysis predicted that a Ca2+-dependent hyperpolarization pathway may play a role in slow-wave sleep and hence in the regulation of sleep duration. To experimentally validate the prediction, they analyzed 21 KO mice and found that impaired Ca2+-dependent K+ channels (Kcnn2 and Kcnn3), voltage-gated Ca2+ channels (Cacna1g and Cacna1h), or Ca2+/calmodulin-dependent kinases (Camk2a and Camk2b) decrease sleep duration, while impaired plasma membrane Ca2+ ATPase (Atp2b3) increases sleep duration. Pharmacological intervention and whole-brain imaging validated that impaired NMDA receptors reduce sleep duration and directly increase the excitability of cells. Based on these results, we propose a hypothesis that a Ca2+-dependent hyperpolarization pathway underlies the regulation of sleep duration in mammals.
So, it seems to the present author that for sleep that K+ efflux is required. This is confirmed by Hodge (2020). https://www.frontiersin.org/articles/10.3389/neuro.02.013.2009/full Hodge states that ‘ion channels are the determinants of excitability; therefore, manipulation of their levels and properties provides an opportunity for the investigator to modulate neuronal and circuit function. There are a number of ways to suppress electrical activity in Drosophila neurons, for instance, over-expression of potassium channels (i.e., Shaker Kv1, Shaw Kv3, Kir2.1 and DORK) that are open at resting membrane potential. This will result in increased potassium efflux and membrane hyperpolarisation setting resting membrane potential below the threshold required to fire action potentials.’
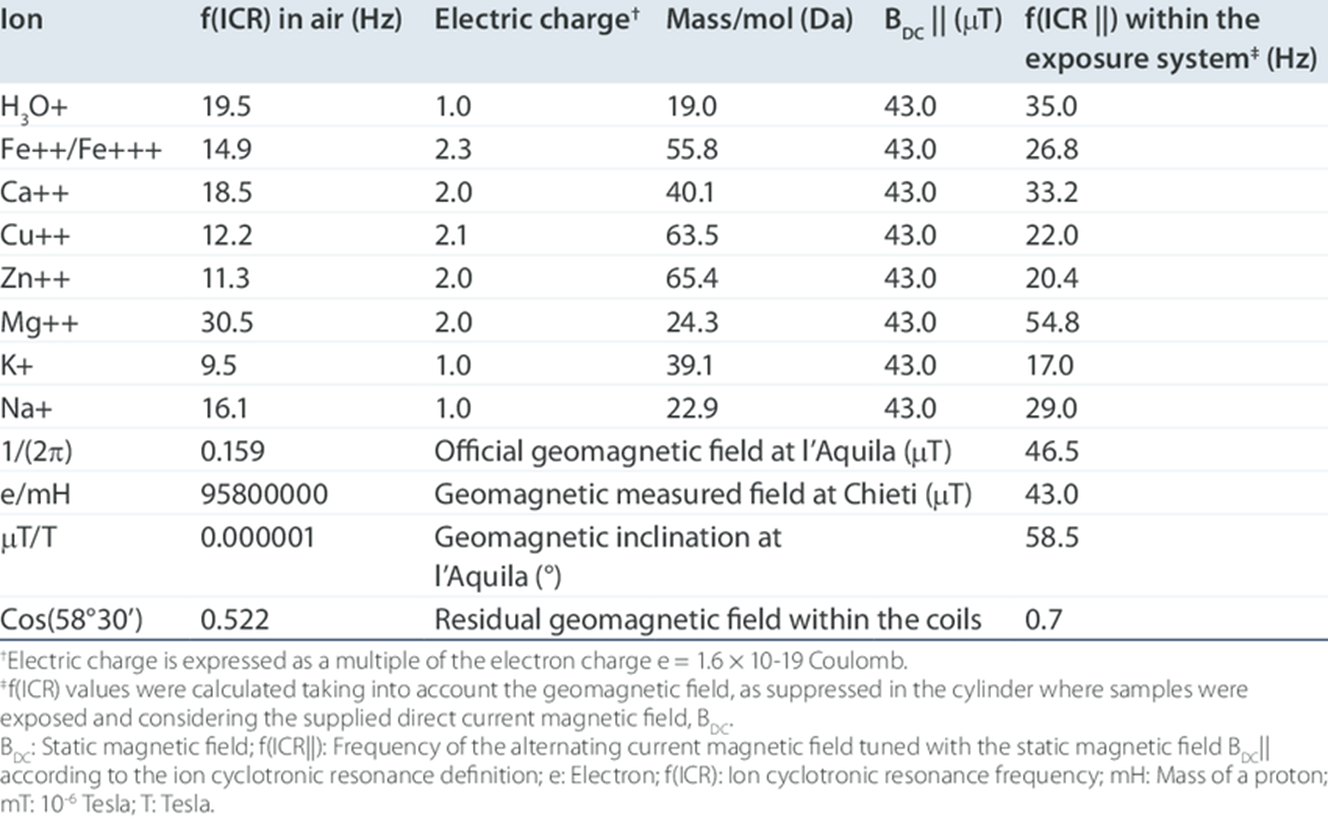
It is relevant thus to enquire if any of Pasche’s sleep frequencies are related to Potassium ICR ( efflux). The Table below shows known ICR frequencies for some common ions at a GMF of 43 micro-Tesla.
Parkinson and Hanks (1989) quote Ca2+ ICR as 38.5 Hz at 50 micro-Tesla. Sakhnini (2007) quote Ca2+ ICR as 28.3 Hz 20 micro-Tesla.
According to the theory, the maximum of the biological effect of CMF
appear when the following condition is fulfilled: the frequency of
the alternating component must correspond to the resonance frequency
of the particular ion, i.e. Ca2+, K+ or Mg2+, according to the
equation
 where fn is resonance frequency, Hz; q is the charge of the ion,
C; m is the mass of the ion, kg; BDC is the value flux density of the
static magnetic field, μT; n is an integer.
where fn is resonance frequency, Hz; q is the charge of the ion,
C; m is the mass of the ion, kg; BDC is the value flux density of the
static magnetic field, μT; n is an integer.
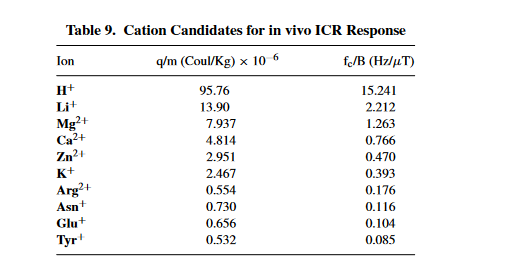
Liboff http://eknygos.lsmuni.lt/springer/17/189-218.pdf suggest that the Charge-to-Mass ICR Signature in Weak ELF Bioelectromagnetic Effects ratio (q/m) and the magnetostatic field intensity B: ωc = (q/m)B. They analyse literally hundreds of known experimental results for ICR ions and magnetic field ‘tuning conditions’ and hence provide the following summary table:
Given the affiliations of the various contributors to the sleep studies and multiple locations referenced in California and in Switzerland for example, it has been difficult to pin down the precise value of GMF. However, the best I can conclude is that the modulation frequency at 42.7 Hz is associated with Ca2+ and that at 21.9 Hz is associated with K+. . The frequency of 2.7 Hz appears possibly to be associated with the first sub-harmonic of Tyrosine+. LAT transporters are known to play an important role in sleep. https://academic.oup.com/sleep/article/41/10/zsy137/5054580. In the 2013 paper, Zimmerman states that 42.7 Hz, has a sleep-inducing effect in healthy subjects. However, administration of the same signal to patients with insomnia did not yield any therapeutic benefits. In contrast, administration of a combination of the four frequencies most commonly identified in patients with chronic insomnia (2.7 Hz, 21.9 Hz, 42.7 Hz, and 48.9 Hz resulted in significant improvements of total sleep time and sleep latency as assessed by polysomnographic evaluation. Thus, I conclude that the 27 MHz AM is certainly influencing small ions by ICR and I further conclude that in the case of insomnia K+ efflux may be being caused or enhanced by the system.
It is worthy to comment that some have challenged the physical reality of ICR, for example Halle ( 1988). However, a critical study by Liboff using radio- labelled Calcium -45 sheds strong confirmatory light on the ICR theory. Wherein a confirmation that the charge-to-mass ratio was explicitly involved in this effect was obtained when Liboff substituted isotopic 45Ca for “Ca in a study on lymphocyte proliferation, showing that the frequency where the maximum ICR effect on proliferation occurred was shifted down by a factor of 12%, exactly what is to be expected for a change of mass of 5 parts out of 40 (Liboff et al., 1987). The angular cyclotron frequency is defined as co =- (q1m)130, where q and m are the charge and mass of the ion, and Bo is the DC field. This work in ICR opened a new line of research in studying the interactions between EM fields and living things. Moreover, all of my own recent experimental work at http://gro-wave. co.uk is supportive of ICR theory.
I will now similarly try to assess the TTF frequencies for cancer. This is far more difficult because the preliminary clinical trials for HCC Liver Cancer appear to have been done in Sao Paulo Brazil and thus, I can only assume that this study gave rise also to the TTF’s filed in the patent. The only one of these frequencies which looks remotely like a ‘traditional’ ICR frequency is the 86 Hz frequency. Assuming a GMF of around 25 micro-telsa yields an ICR of 3.44 per micro-Tesla. No such listing exists, but the closest listing is the 3rd harmonic of the Mg2+ ion ICR. Reverse correction of a more appropriate ratio yields 22.4 micro-Tesla as the operative GMF in Sao Paulo. In my earlier theoretical work I calculated a slightly higher value of GMF around 26 micro-Tesla.
It is well known that magnesium and its transporters have complex relationships in cancer, see Wolf and Trapini (2012), https://portlandpress.com/clinsci/article-abstract/123/7/417/69076/Magnesium-and-its-transporters-in-cancer-a-novel.
Liboff does state that higher harmonics of ICR frequencies are possible but only references up to about the 5th harmonic and literature searches of the available experimental work seem to suggest the same. Liboff further states that higher harmonics of ICR frequencies can be expected to excite multiple ions simultaneously.
Thus in order to account for the other TTF’s in the KHz range and the demodulation effects at CAV 3.2 leading to changed pulse and blood pressure in the test subjects at least some new development of ICR frequency will be required. Moreover. the TTF frequencies observed are of significantly higher Q than those of lower frequency ICR experiments. Barnes has supplied this elsewhere, but the theory is also summarised below. For instance low frequency ICR resonances appear to have a Q as low as 10 whereas the Q’s described for TTF’s appear to be at least 3 orders of magnitude greater.
Development of ICR theory to account for the observation of multiple KHz TTF frequencies of higher Q than traditional ICR and both CAV3.2 enhanced calcium influx and demodulation.
The average GMF (geomagnetic field) in the USA is some 47.5 micro-tesla. I therefore constructed table 1 below to show the ion cyclotron resonance parameters of all the common biological ions, most taken from Bioengineering and Biophysical Aspects of Electromagnetic Fields (Handbook of Biological Effects of Electromagnetic Fields)20 Oct 200 by Ben Greenebaum and Frank S. Barnes ( Chapter 9 Liboff) also found at http://www.sibeonline.com/download/Liboff%20-%20ICR%20interactions%20in%20living%20systems%20-%20SIBE%202013.pdf. Following this reference, I have obtained the fc/B values for certain tabulated ions and the rest I have calculated from their charge and molecular weights. I have then divided those fc/B values into the given values of tumour treating frequency. When treated in this way each tumour frequency appears about two orders of magnitude higher than expected ICR frequency. One possible explanation for this is that ICR theory needs to be amended to take into account dielectric constant and/or viscosity. I would predict a quasi- harmonic behaviour for each ion if its angular momentum is to be conserved as it descends through the selective filter and into the hydrophobic core. In other words when the ion is in a totally hydrophobic channel environment it will seem has though it has lost mass or waters of hydration. I believe this argument to be justified as follows.
Biological ion channels are nanoscale transmembrane pores. When water and ions are enclosed within the narrow confines of a sub-nanometer hydrophobic pore, they exhibit behaviour not evident from macroscopic descriptions. At this nanoscopic level, the unfavourable interaction between the lining of a hydrophobic pore and water may lead to stochastic liquid vapor transitions, see Aryal et al (2014). These transient vapor states are de-wetted , i.e. effectively devoid of water molecules within all or part of the pore, thus leading to an energetic barrier to ion conduction. This process, termed hydrophobic gating was first observed in molecular dynamics simulations of model nanopores, where the principles underlying hydrophobic gating (i.e., changes in diameter, polarity, or transmembrane voltage) have now been extensively validated.
Previous observations of ICR have been in solution. Calcium ICR can exhibit hyperfine splitting effects due to hydronium and hydroxyl, see for example but not exclusively Sheykina 2016.
‘Characterisation of weak magnetic field effects in an aqueous glutamic acid solution by nonlinear dielectric spectroscopy and voltammetry.’ It is my contention that when experimenters have attempted to apply ICR frequencies in biological situations they have used these solutions determined frequencies which are those of hydrated ions. Whereas they may be a handful of biological situations where this is relevant (refs) it is clearly not the case here. There is another essential difference also. The Q-factors observed for ICR elsewhere are low. The bandwidth is of the order +/- 10% of the fundamental frequency. In the TTF case here Q values of apparently between 10^4 and 10^5 are seen at least in terms of the requirement to produce biofeedback. I will show that the difference can be understood in terms of the difference between bulk and structured water, ion cages and dehydration following for example Del Giudice. Pazur (2018) also considers calcium ICR in water cages and finds the oscillations of the Belousov–Zhabotinsky chemical reaction are significantly reduced under Ca²⁺ ICR application. Secondly an “oscillator” of calcium ions appears to be able to itself couple coherently and predictably to large-scale coherent regions in water. This system appears able to regulate ion fluxes in response to very weak environmental electromagnetic fields. See Fulltext http://www.tandfonline.com/eprint/KYKEqMetHpz7sKwakZct/full.
f ( 27.065) Brazil average
A picture containing background pattern Description automatically generated
The ratios of frequencies observed from the TTF’S (modulation frequencies applied to 27 MHz carrier) reference potassium as a base frequency are highly compatible with the ratios obtained from the more classically reported Ion Cyclotron resonance frequencies. Although it is believed this has never been attempted by any authors or research groups previously, it is relatively easy to account for the high harmonic content observed. Several have commented that ICR cannot properly apply in the hydrated case. There are strong viscous forces on the ion. Indeed, Halgamuge et al (2009) have highlighted the signal to noise ratio problem with the basic ICR model and has also noted that theoretically true ICR did not ought to be able to occur for ions in a viscous medium at frequencies below about 2000 Hz due to the number of collisions per second they are encountering. Lednev ( ref) amended the ICR model and came up with the IPR model which overwhelms the SNR problem and has similar predicted frequencies. The same mathematical prediction can be obtained using a different theoretical approach: the analysis of the velocity of the damped ion under the influence of the Lorentz force, see Vincze et al (2008). In both cases, the prediction of a dependence on specific values for B AC/B DC has been tested in several experiments.
Liboff and McLeod (1988) first considered the cyclotron resonance model for channel ion transport in weak magnetic fields is extended it to include damping losses. Their model leads to discrete modes of vibration (eigenfrequencies) in the ion‐lattice interaction, such that ωn = nωc. The presence of such harmonics is compatible with recent results by Blackman et al. [1985b] and McLeod et al. [1986] with the interesting exception that even modes do not appear in their observations. Especially relevant to the present interpretation in my work, their model has no restriction whatsoever on n. Further their harmonic formalism is also consistent with another reported phenomenon, that of quantized multiple conductances in single patch‐clamped channels.
Liboff et al (2106) have made recent observations of low-frequency electromagnetic oscillations in water which suggest an inductive structural component. Accordingly they assumed a helical basis enabling them to model water as an LC tuned oscillator. A proposed tetrahedral structure consisting of three water molecules and one hydronium ion was incorporated into the Boerdijk-Coxeter tetrahelix to form long water chains that are shown to have resonance frequencies consistent with observation. Their model also serves to explain separately reported claims of ion cyclotron resonance of hydronium ions, in that the tetrahelix provides a built-in path for helical proton-hopping. For this reason I shall include hydronium ions in my list of biological ions for later analysis of Zimmerman and Pasche’s data.
If I take the LC model, it is logical to suppose the resonant frequency may depend inversely on the square root of the dielectric constant. Thus as we descend into the hydrophobic region epsilon falls from 80 to as low as 2-6. If ICR or ICR like and water cluster resonance cohere, as has been suggested by Del Giudice (ref) we should expect an increase of up to 7 fold in frequency. If the angular momentum of the ion entity is conserved I would similarly expect a frequency to be proportion to the inverse of the square root of the effective radius. For a loss of 6 water molecules this represents approximately a five fold increase in frequency. Much larger water clusters are reported in biological systems so theoretically this could easily double. For example, often the binding of two protein molecules seems to be mediated by clustered water. It is known, for example, that the crystal structure of trypsin and trypsin inhibitor don't fit together perfectly and the amino acid side chains conflict. In order to form a tight complex, these side chains must change their conformations. Mobile water structures along the proteins' surfaces link the two proteins by binding to each. To do this these water structures are organized as fragmented dodecahedrons (12-sided figures), 9–15 Ångstroms long, enough to accommodate 30 or more molecules. There are similar events in the biochemistry of myoglobin.
Combining the dielectric constant idea and the conservation of angular momentum could thus easily account for the observation of an ICR frequency some seventy times higher than expected. Previously ICR harmonics as high as about 15 have been reported, see for example Pazur (2004) who note ICR for glutamic acid at 4.14 Hz but note other frequencies worthy of remark are 62, 78 and 94 Hz, being four folds of the used base ICR resonance frequency 4.14 Hz.
Further, I would perhaps expect there to be special conditions where higher harmonics still could match the ICR frequency of more than one type of ion simultaneously as in, for example, their lowest common multiple. Since Zimmerman and Pasche’s biofeedback frequency registration technique relies on stimulating excitable tissue, I would naturally expect these ‘LCM’ conditions to produce a strong stimulus. Under such special conditions one may well have frequencies which drive these ICR’s in phase with mechanical resonance of other structures within cells or their organelles.
Furthermore, due to the vast number of different types and families of ion channels in biology I would expect an almost pseudo-random distribution of harmonics of each specific ion’s ICR Frequency depending on type of channel, size and shape of the selective filter and pitch of the helices involved. For example, some channels are more conical than others. In fact, this is exactly what the data shows.
It is well known that the components of ion channels execute coupled movements, see for example Horn ( 2002). For example, there has to proper co-ordination between the S4,5 and 6 sub-units in the open and closed states. There is experimental evidence to suggest some of these movements are rotational, see Horn (2000).
Thus, the channel itself or its various sub-units will have finite angular momentum and will hence behave as a harmonic oscillator.
Placing additional angular momentum on the traversing ions by means of ICR at its fundamental or harmonic frequencies will lead to superposition behaviour effectively there will be regions of motional enhancement and regions of motional restriction depending on the harmonic frequency. Due to the very precise structure and bonding requirements in a moving ion channel it is plausible to visualise how high Q responses within phase and antiphase dehydrated ion motions might be achieved.
Previous discussions of the interaction of EMF and biology has only considered ion channel enhancement (refs). Electromagnetic fields act via activation of voltage‐gated calcium channels to produce beneficial or adverse effects, see Pall et al (2013). Usually, only calcium channels either inwardly or outwardly rectifying voltage gated types have been considered (refs). Hence it has been stated and experimentally shown in some cases that application of ELF ( refs) or even modulated 147 MHz ( ref) causes increased calcium efflux/influx ( check refs). The ICR or similar models have been used to explain this on the grounds that ions on the membrane surface and close to pore entrances are encouraged en-route as it were. Influx or efflux is encouraged depending on the type of ion channel and the initial membrane or ligand surface concentration of ions. The frequencies or modulation frequencies employed have exclusively been low ( Hz or tens of Hz). There is sufficient body of scientific evidence to suggest that application of calculated ICR frequencies has real biological effect, with one of the earliest and most profound papers being that of Smith and Liboff et al ( 1987) dealing with Calcium Cyclotron Resonance and Diatom Mobility. This is elegant because it shows downstream effects of ICR controlling simple molecular machinery.
There is also evidence from the field of plant biology. Smith et al (1995) tested the ion cyclotron resonance theory of electromagnetic field interaction with odd and even harmonic tuning for cations on seeds of Raphanus sativus, var. Cherry Belle. The seeds were exposed to combined parallel static and sinusoidal 60 Hz, 40 μT peak-peak ac fields turned to the fundamental, 2nd and 3rd cyclotron resonance harmonics for calcium and potassium ions. Other seeds were exposed to similar fields tuned to the fundamental and 5th harmonic for magnesium. Concurrent controls consisted of seeds exposed to the ac field only, and to ambient geomagnetic and stray 60 Hz ac fields. After 21 days plant height, aboveground weight, root weight, stem diameter, leaf length, leaf width and length/width aspect ratio were measured and compared to in-group controls. Calcium slowed germination, potassium speeded it, and magnesium left it unaffected. Calcium and magnesium tunings were generally stimulatory to growth, while potassium tuning was inhibitory, except for root weight. Controls (ac only) were unchanged from the ambient field controls. Fields at the 2nd harmonic were ineffective, except for potassium 2N, which appeared similar to a weak calcium effect.
Comisso et al (2005) studied dynamics of the ion cyclotron resonance effect on amino acids adsorbed at the interfaces. They reproduced the Zhadin experiment, which consists of the transient increase of the electrolytic current flow across an aqueous solution of L‐arginine and L‐glutamic acid induced by a proper low frequency alternating magnetic field superimposed to a static magnetic field of higher strength. Further they identified the mechanisms that were at the origin of the so‐far poor reproducibility of the above effect: the state of polarization of the electrode turned out to be a key parameter. The electrochemical investigation of the system shows that the observed phenomenon involves the transitory activation of the anode due to ion cyclotron frequency effect, followed again by anode passivation due to the adsorption of amino acid and its oxidation products.
The relevant conclusion here was that there will be the likely occurrence of similar ion cyclotron resonance (ICR) phenomena at biological membranes and hence the implications not only for common small ion circulation but also for amino acid circulation in living matter under the consequent impact of environmental magnetic fields.
A useful analogue for ion channelling and downstream control is to imagine the building a six-mile-high dam around the deepest part of the ocean. Now picture what a cell does when it reduces calcium ions to 20,000-fold lower levels inside the cell than surrounding the cell. Uncontrolled Ca2+ leaks induce cell death, whereas controlled Ca2+ entry triggers an enormous array of actions, ranging from secretion to cell division
Ion channels are the electrical switches that control these actions. One ion channel directs the flow of ~10 million ions per second, in turn rapidly changing intracellular Ca2+ levels. The human genome contains more than 300 genes encoding ion channels, effectively these are the cell's transistors
Although demonstrated in plants few are probably unaware of ICR effects in mammalian and human biology under the influence of environmental fields other than what has been reported on Calcium channel effects. Hence probably why Elnasharty et al suggest that the potassium channel too may be a target for electronic modification as though this in itself were a rather radical proposition.
However, I will show herein that not only a numerous different voltage and ligand gated ion channels for all common biological ions are affected by the Zimmerman and Pasche TTF’s but also and for the first time, that high harmonics of ICR act in a manner contrary to that associated with ELF application. In other words, under some conditions Ca2+ entry can be slowed rather than accentuated. This is entirely consistent with both the angular momentum hypothesis and the dehydration hypothesis above. Using the same experimental data due to Zimmerman and Pasche, I will also show that high ICR harmonics also effect amino acid transporter channels too. Finally, I will also show that under some conditions K+ can also be suppressed.
There has been comment by Teplan et al ( 2017) that the Q factors seen with Pasche and Zimmermann’s TTF’s are unrealistically high. However, if one treats the system as a mechanically resonant system with viscoelastic damping and considering the de-wetting phase of ions one can consider the transition from water to vapour viscosity.
Evaluating the resonance condition, one arrives at Qv/Qw = Eta w/ Eta v
And it is also known that the viscosity and viscous shear forces in nanoconfined water can be orders of magnitudes larger than in bulk water if the confining surfaces are hydrophilic, whereas they greatly decrease when the surfaces are increasingly hydrophobic. This decrease of viscous forces is quantitatively explained with a simple model that includes the slip velocity at the water surface interface, see Ortiz-Young et al (2013).
The two processes above are sufficient to account for the high Q’S observed.
Detailed interpretation of the Zimmerman and Pasche frequencies.
Because the geomagnetic field in Sao Paulo is estimated to be between 20-30 micro-Tesla it is not appropriate to develop a detailed interpretation either from Table 1 above or by normalisation because the field will vary on a day by day basis. I thus considered in much greater detail the downloadable files, there are three of which, described as; Breast tumour treating frequencies, http://drchrisbarnes.co.uk/BREAST.pdf and HCC (liver) treating tumour frequencies. http://drchrisbarnes.co.uk/HCC.pdf and Random frequencies which did not provoke effect, http://drchrisbarnes.co.uk/RAND.pdf. These files are used as follows;
The extreme left column is the so called TTF ( tumour treating frequency as identified by the reflex response of the patient directly or by physiological monitoring of changes to patient vital signs such as heart rate and blood pressure. The remaining columns are the precise ICR frequencies and harmonics for the known common biological ions and common amino acids at the GMF according to hydrogen. Where there are precise or extremely close numeric (frequency) matches between the TTF and the ICR harmonic this has been indicated/highlighted in green. Lesser matches in yellow and lesser matches still in orange. No match is just left as bare print, black on white.
Plugging in a value of 25uT for the GMF yields approximately 380 Hz for the first ICR value of the proton. In the ‘breast’ file the nearest frequency to this is 414.817 Hz. In the HCC file the nearest frequency 410.231 Hz. I thus interpret these frequencies as being the fundamental ICR for protons and I interpret the differences not as ‘patient specific’ as suggested by Zimmerman and Pasche et al but rather simply being due to a difference in the local GMF when the treatment was given. Accordingly dividing these two frequencies by Fc/B ( 15.24) for the proton yields the precise value of GMF in each case, namely 27.21895858 uT in the Breast file and 26.91804 uT in the case of the HCC file. I the utilise these GMF’s to calculate the expected fundamental ICR frequencies for a significant number of other common relevant biological ions including: H+, Li+, OH- , H3O+, Mg2+, Ca2+, Na+, Zn2+, Cl-, K+ and a number of small amino acids. I then divide these fundamental frequencies into each of the stated 194 TTF frequencies to find the harmonic number for each ion. I define a harmonic as being valid if it falls as an integer or close thereto. For higher harmonics I allowed a maximum deviation of +/- 0.1 on the harmonic number. I then count the number of harmonics for each specific ion which fulfils this chosen condition. I have set no upper bound on harmonic number but essentially my chosen precision gets sharper and sharper in an arithmetic progression. The results are available in XL spreadsheets. Proton ICR harmonics from 1-45 are observed. Much higher harmonics of heavier ions and amino acids are observed, tantamount with the dehydration hypothesis above.
The random file contains 237 random frequencies and it is stated none are closer than .5 Hz of an actual treatment frequency. For the random file I took the GMF as being the average of the GMF for the two treatment files. I used the same criteria for the definition of an ion specific ICR harmonic. The result is available in an XL spreadsheet.
For all three files I then went on to calculate the percentage of frequencies that fulfilled ICR or ICR harmonic conditions for each specific ion and have showed these results in a separate spreadsheet, an extract of which is included in the table below:
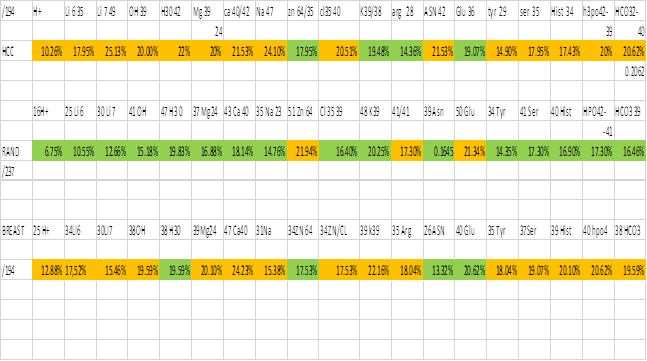
I have used green to represent a low or lowest percentage for the tabulated ion and orange to represent high and highest percentages. It can be clearly seen that the ions which give rise to action potentials in excitable tissue have more ICR harmonics in the treatment files than in the random file. This is totally consistent with perturbation of ions, their channels, the ICR resonance condition and /or a downstream event being the cause of the biofeedback registration in the treatment cases and the lack of registration upon application of random frequencies. There are also some far more profound observations which I will discuss later in this present paper. I also considered hydrogen polarisation models, see and was unable to fit the results in any way, see Halgamuge et al (2009) .
Can CAV3.2 ion channel modulation explain Zimmerman’s results for pulse changes and the obeserved cancer Biology?
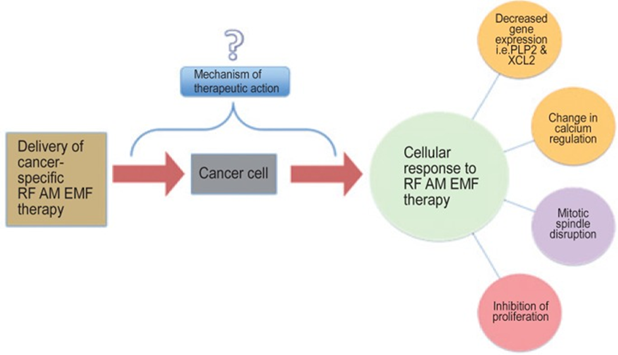
Zimmerman et al in their original work categorically state that there are known known mechanisms for their results which sadly downplays their excellent work and makes their system less likely to be commercially exploitable.
Human nature tells us if you buy something you want to know how it works. Like a drug you don’t know how or why it works then it could simply be placebo! I have included Zimmerman’s graphic to show where they are at. Of course, things have changed somewhat now with the identification of the CAV 3.2 channel by Jimenez as the site of action of this technology.
Certainly, for the breast cancer file above, significantly the largest number of acceptable harmonics in the file 24.2% are associated with calcium. The figure being slightly lower for the HCC file. We should not, however, lose sight of the fact that there are numerous ion channels in excitable tissue and the channels in addition to simply CAV3.2 seem to be giving rise to the pulse changes measured. Indeed other notable ion channels and their high harmonics especially those of sodium, potassium and magnesium also appear to be contributing about 20% each to the total TTF frequency count. I feel sure eventually it will be shown that channels are as genetically diverse almost as humans themselves. Already several hundred different ion channels have been discovered. Although ion channels are found mainly in excitable cells, they are also hallmarks of cancer each type of cancer has almost its own unique ‘onchochannelopathy’ see for example, but not exclusively, Litan and Langhans (2015).
The next question I would pose is to enquire if CAV3.2 is sufficient to give rise to all the cancer biology observations made. Phan et al (2017) has identified the complete family of voltage gated calcium channels as interesting targets for cancer therapy. Ca2+ oscillation is a system-level property of the cellular Ca2+-handling machinery and encodes diverse physiological and pathological signals. The study of Sun et al (2019) tests the hypothesis that Ca2+ oscillations play a vital role in maintaining the stemness of liver cancer stem cells (CSCs). Cancer cells are very cunning and can remodel the whole of their Calcium transport and metabolism systems. Thus, there is much recent interest in Ca2+ transport-targeting tools for cancer diagnosis and treatment, see Prevarskaya et al (2014). A very comprehensive review of calcium signalling in cancer is given by Xu (2018). CAV3.2 is known to have conflicting types of effects in breast cancer. High levels of Cav3.2 were associated with poor outcome in patients with oestrogen receptor positive (ER+) breast cancers, whereas Cav3.2 levels were correlated positively with patient survival after chemotherapy in patients with HER2-positive breast cancers, see Pera et al (2016). In HCC, the deregulation of the Ca2+ transportome contributes to tumorigenesis, the formation of metastasizing cells, and evasion of cell death. In this review, we reflect on these aspects by summarizing the current knowledge of the Ca2+ transportome and overviewing its composition in the plasma membrane, endoplasmic reticulum, and the mitochondria, see Lai et al (2022).
Considering first XCL2 ( chemokine) . XCL2 encodes for a protein that enhances chemotactic activity for lymphocytes and downregulation of XCL2 has been shown to be associated with good prognosis in patients with breast cancer (Teschendorff et al, 2007; Teschendorff and Caldas, 2008). Activated chemokine receptors triggers a variety of effector pathways, including calcium signalling, generating an intracellular calcium ion flux and causing chemotaxis and cell trafficking. Jimenez has showed RF AM activation of CAV 3.2 alters intra-cellular calcium and hence I propose results in the XCL2 knock down observed. In reality complex pathways such as P13 K/AKT/NF-κB and MAPK/ERK could be involved.
PLP2 is endoplasmic reticulum-based integrated ion channel. Its knockdown drives better outcomes in cancer. I suspect that TTF’s change PLP2 directly or by ER stress. See King (2020).
I conclude that the involvement of TTF’s with CAV3.2 influx as cited by Jimenez is a real effect in both the TFF determination itself through pulse/blood pressure changes and the anti-cancer activity. However, based on my theoretical analysis I cannot conclude it is the only anti-cancer effect at work.
The mechanism of the pulse/blood pressure effect.
CAV3.2 and many other families of voltage gated ion channels and transporters are ubiquitous in excitable tissue. In order for the patients to feel a ‘jolt’ in pulse change when the TTF modulation frequency is appropriately ‘tuned’ there must be a coincident change in nerve action potentials. I have no reason to suppose that CAV3.2 could not bring about such a change but neither do I have a reason to suppose that other voltage gated channels would not be able to achieve the same or similar. In other words, not every frequency that is listed as a TTF may be a frequency that changes ion flow in CAV3.2. In order for such change to occur, the cell membrane and its channel must effectively act as a rectifier, and demodulating the incoming signal. The difference between this an a rectifier in the normal sense of the word is that normally a rectifier would not be frequency selective over narrow ranges. We thus need to search the literature to see if such rectification is indeed possible. Moreover, given that voltage gated ion channels are ubiquitous throughout the eukaryotic world, I have been able to include some plant based experiments courtesy of gro-wave UK to further elucidate the matter.
Demodulation
In a paper entitled ‘A breakthrough in Cancer Treatment or Cancer cell proliferation is inhibited by specific modulation frequencies but how and why?? Some new findings by Dr Chris Barnes, Bangor Scientific and Educational Consultants, Wales, UK. and a comprehensive but totally independent explanation of the new cancer treatment device used by Zimmerman et al (2013)’ first published online 2018, I discussed the possibly of AM demodulation by ion channels.
How can modulated RF radiation influence ion channels anyway?
Galvanovskis and Sandblom (1197) showed that even very weak low-frequency electromagnetic signals (<100 Hz and down to 100 microT) may be detected in a cellular system with a large number of ion channels. But what is the evidence for the detection of such systems with higher frequencies or modulated signals?
Bawin and her coworkers have reported changes in binding of calcium after exposure of avian brain tissue to nonionizing electromagnetic radiation. Blackman et al ( 1979) used the forebrains of newly hatched chickens, separated at the midline to provide treatment‐control pairs and labelled them in vitro with radioactive calcium. Samples of tissue were exposed for 20 minutes in a Crawford irradiation chamber to 147‐MHz radiation, which was amplitude modulated sinusoidally at selected frequencies between 3 and 30 Hz. Power densities of incident radiation ranged between 0.5 and 2 mW cm−2. Compared with nonirradiated samples, a statistically significant increase in efflux of calcium ions (P < 0.01) was observed in irradiated samples at a modulation frequency of 16 Hz and at a power density of 0.75 mW cm−2. Their data confirmed the existence of the frequency “window” reported by Bawin et al., as well as a narrow power‐density “window” within which efflux of calcium ions is enhanced. Such frequency windows can be interpreted in terms of Ion Cyclotron Resonance (ICR).
Habash, Electromagnetic Fields and Radiation: Human Bioeffects and Safety (2018) , describes numerous other examples.
Ramachandran ( 2007) has shown experimentally that voltage gated ion channels are capable of responding to an 800 MHz RF carrier wave effectively by a process of rectification due to the combination of membrane capacitance and non-linearity in the channel itself.
D'InzeoStefano et al (1993) has discussed a stochastic model of Ionic channel gating under electromagnetic exposure. They considered the membrane channel as a non-deterministic state machine. Its behaviour is fully described by a set of states, a matrix of transition rates, and a vector for the probability of the machine to be in each single state at a certain instant. A stochastic model was developed, generating random processes where the probability for each state is an aleatory variable. The model was tested for both voltage gated and ligand-dependent channels, both unexposed and exposed to EM fields in the ELF range.
Intuitively, I would propose that rectification or demodulation of a modulated HF carrier wave would occur at cell membranes and hence expose ion channels to the modulation envelope frequency component. Indeed, there is evidence to support my claim. Elnasharty et al discuss ‘cell membrane analysis using modulated electrophoresis. They describe method of examining this low-frequency region using a low frequency signal to modulate a 1 MHz carrier wave, allowing membrane conductance due to conduction through ion channels and surface conductance of the membrane to be probed in this unusual way for the first time. They produce DEP spectra before and after the application of ion channel blockers.
The technique works because demodulation of the AM signal occurs. The simplest demodulation circuit for amplitude modulation signals consists of a diode and a capacitor. In a suspended cell, the membrane acts as a capacitor, while there are two methods in which ion channels can act as diodes to demodulate the signal.
Ion channels will normally conduct along a concentration gradient of the particular ion they transport. If there is a much higher concentration of ions inside the cell than outside the cell ( or vice versa) making the flow of a particular ion essentially one direction similar to the flow of electrons through a diode. Additionally, some ion channels move ions directionally have an intrinsic selectivity filter only allowing excreting or taking up a particular ion and thus relative to total potential ionic current as a whole behave as a diode even without a concentration gradient. Since an ion needs a characteristic time to be transferred though a particular ion channel, the electric field will only have an effect on ion channels that transfer change in less than half the period of the signal. This has been modelled as an inductive component in then ion channels response for some time and gives rise to resonance conditions at well-defined frequencies. Although Elnasharty et al only focus on the electric field, I conclude that the magnetic field will similarly exhibit resonance effects due to ion cyclotron resonance. These resonance peaks should be detectable in the DEP response of the cell. If the amplitude of a high-frequency carrier wave is modulated using a lower frequency signal, then I would anticipate that where there is a change in conductance to due to ion channel activity, the net force on the cell would be due to the superposition of the low-frequency signal acting across the membrane due to the demodulation effect, plus the effect of the high-frequency signal. This force will also be felt by any piezo channels present in the cell. This high frequency component will depend solely on the interaction between the medium and cytoplasm, the membrane having been bypassed at these frequencies. It is therefore possible to deduct the high-frequency force component by measuring the force acting on cells when exposed to an unmodulated signal at the carrier frequency. Hence, by using a low-frequency signal modulated onto a MHz frequency carrier signal. This is what allowed Elnasharty et al to observe the DEP spectrum of cells at low frequency and observe changes to the spectrum when channel blockers and other chemical agents were used. They observed frequency peaks both in the low tens of Hz and at about 1Khz. The precise frequencies depended on the nature of the channel blocker and/or ionophore.
The work of both D'InzeoStefano and Elnasharty is useful in that it provides a viable physical mechanism for interactions of modulated radio frequencies and biology of which there are lots of experimental observations but few viable explanations. Whereas essentially their work is interpreted in terms of electric field gating and component we must never forget that in an EM wave the magnetic component is inseparable. Both are candidates for demodulation. We only have to research the earlier pioneers of radio and the magnetic coherer which preceded the cat’s whisker to understand this. Moreover, I will show later there are potentially fewer objections in terms of signal to noise ratio in the magnetic case.
Liboff has stated that ICR is just as relevant to plant ion channels as it is to animal systems and has provided references. Indeed, the present author has been exploiting ICR based devices to enhance plant growth, see http://gro-wave.co.uk.
When modulated RF energy AM modulated at fundamental ICR frequencies was applied to grafted tomato plants in a rock wool growing medium the following data was obtained.
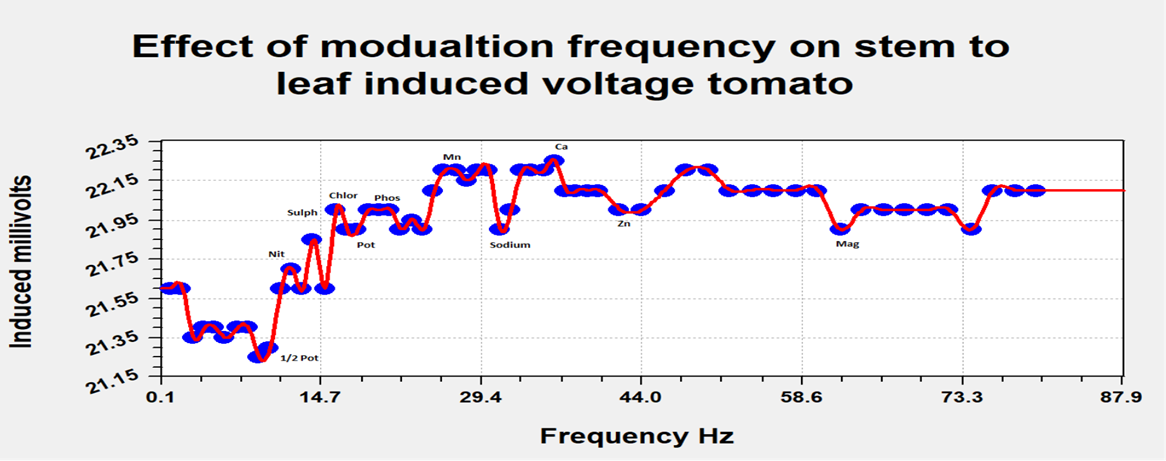
In a separate experiment a Traescantia plant was exposed to a 40 MHz AM modulated signal, modulated at typical frequencies in the range used by the TheraBionic cancer therapy system. Exposure was by means of short insulated wire loop antenna in the region of an upper leaf of the plant. The lower part of the stem was connected directly to the high input terminal of a simple PC audio amplifier via a needle electrode, grounded at the soil in the plant pot. Weak amplitude audio emissions could be heard in the speaker but only at very specific modulating frequencies. There were eighteen measurable frequencies spanning the range 944Hz to 11.34 KHz. Including a frequency of 1.45 KHz.

In yet a further experiment, the RF transmitter was replaced by an AM modulated LED light source. In this case audio was only discernible in the region of the 1.45 KHz peak.
The above has provided by theoretical and experimental grounds for the highly frequency selective demodulation process in ion channels as a real process and given the induced jumps in voltage above could well be one that gives rise to changed pulse rate and/or blood pressure in the patients in the Therabionic cancer study.
Discussion, conclusions and other relevant work
In conclusion then I have shown a plausible mechanism by which voltage gated channels in cellular membranes can behave as frequency selective demodulators. Moreover, I have shown experimental results in plants which demodulate frequencies in a very closely similar range to those of the Therabionic study. I conclude that the Therabionic pulse effect is a real effect with a real demodulation mechanism. Further and of somewhat related interest, Liguori (2022) has recently demonstrated whole body resistance effects when either acupuncture points are stimulated or when ICR frequencies are applied. Water with incoherent phase boundaries is a bio-mimic of the cellular membrane situation. Pazur (2017) comments on the fact that weak magnetic and electromagnetic fields affect physiological processes in animals, plants, and microorganisms. Ion cyclotron resonance (ICR) is discussed as one of the sensitive mechanisms, which enable perception of the geomagnetic field and its orientation. Numerous biological effects are observed involving several small ions, showing windows of predicted frequencies and intensities. The pioneering work of Guiliano Preparata and Emilio Del Giudice using quantum electrodynamics showed that spontaneously originating coherent regions in water facilitate ICR effects at incoherent water phase boundaries. Pazur further examined the ICR response of the calcium ion (Ca2+), crucial for many life processes. They used a bio-mimic consisting of an aqueous solution containing the biologically ubiquitous membrane lipid L-α-phosphatidylcholine that serves as a biomimetic proxy for dynamic light scattering (DLS) and nonlinear dielectric spectroscopy (NLDS) measurements. One notable result is that this system approaches a new equilibrium upon addition of calcium by means of the oscillatory Belousov–Zhabotinsky chemical reaction, oscillations are significantly reduced under Ca2+ ICR application. Secondly an “oscillator” of calcium ions appears to be able to itself couple coherently and predictably to large-scale coherent regions in water. This system appears able to regulate ion fluxes in response to very weak environmental electromagnetic fields. Funk (2009) probably sums up the whole situation in one simple statement: ‘The triggers exerted by ion concentrations and concomitant electric field gradients have been traced along signaling cascades till gene expression changes in the nucleus.’ This is both exactly what Therabionic observe with TTF fields and exactly what the present author at gro-wave observes with plant culture.
Field effects
If the above ICR hypothesis stands, geomagnetic field effects ( GMF) ought to be the entire crux of the matter regarding the operation of the Therabionic system and their method of selection of TTF frequencies. These should manifest in several ways:
TTF frequencies ought to vary slightly from day to day according to GMF. In the original 2012 paper Zimmerman certainly states that they vary from patient to patient and it is not clear that all patients were given treatment cycles at precisely identical times. So, this is partially supportive.
The original system was set up and its early clinical trials done in Sao Paulo, Brazil. I would expect very different TTF frequencies in locations with different GMF’s if they are ‘re-tuned’ every time. However, nothing is explicitly stated in the sales literature for the machine.
The machine is also being trialled at various locations in Europe. On the basis of (2) above, I would expect it not to work or not to work as efficiently as in Brazil unless it were ‘re-tuned’ .
As a possible caveat to ( 3) above, the machine has been used in Europe and North America where the GMF field is usually and quite coincidentally about double what it is in Sao Paulo. Given the very high ICR harmonics being employed there may potentially be enough harmonics ( TTF’s) falling onto the CAV3.2 Channel for some kind of operation.
It would be very instructive indeed to have full access to clinical data across ALL the various sites of operation. Only then could the mechanism be completely nailed down.
Given all of 1-5 above, I return to the data I have observed with plants. I do, indeed, notice slight variations ( a few percent) in the demodulated frequencies from day to day. This could potentially be GMF effects but equally potentially it could be hydration effects. I would propose to further future measurements employing a GMF sensor.
Thus with regard to Therabionic technology, although strongly supported, the dehydrated ICR hypothesis will only be fully confirmed when the groups concerned decide to make an exploration of TTF frequency change versus GMF field change.