Is SAR
worthwhile and could our choice of radio and TV broadcasting frequencies be
killing us and what of 600 MHz for 4G?
Abstract
Definitions of
present ways of measuring SAR are given.
Disadvantages of the SAR technique are discussed which highlight the
fact that due to internal resonances some parts of the body could be receiving
far more energy than that defined by SAR and hence either more heating or more
bio-effect. The fact that SAR does not
take bio-magnetite into account may also be important. Causes and types of body resonances to
radio frequency radiation are discussed in more detail and in particular with
regard to the proposed use of 600 MHz as a frequency for 4G mobile telephony in
the UK. Potential hazards of this
frequency to the prostate gland in particular are discussed. Radio frequency
radiation, particularly with pulse modulation, as a possible cause of voltage
gated ion channel modulation is discussed as is radiation as a bio-growth
promoter is also discussed. Reasons for
inconstancies in experiments and epidemiological studies are also visited. It is concluded that for the moment at least
we should always err on the side of caution until we more fully understand humans
as ‘beings of frequency’. In future it
may not only be possible to design our communications systems and their siting
accordingly but also one day we may be able to develop ‘Startrek’
style ‘tricorder’ units to diagnose us and cure us on
the basis of our body response to radio frequency radiation at a cellular
level.
Introduction
The standard way of defining the safety of mobile
telephones and other radio frequency equipment used proximal to the Human body
is so called SAR or specific absorption rate.
Specific absorption rate
(SAR) is a measure of the rate at which energy
is absorbed
by the body when exposed to a radio frequency
(RF) electromagnetic field;
although, it can also refer to absorption of other forms of energy by tissue,
including ultrasound. It is defined as
the power
absorbed per mass
of tissue and has units of watts
per kilogram
(W/kg). SAR is usually averaged either over the whole body, or over a small
sample volume (typically 1 g or 10 g of tissue). The value cited is then the
maximum level measured in the body part studied over the stated volume or mass.
Various governments have defined safety limits for
exposure to RF energy produced by mobile devices that mainly exposes the head
or a limb for the RF energy:
United States:
the FCC
requires that phones sold have a SAR level at or below 1.6 watts
per kilogram
(W/kg) taken over a volume containing a mass of 1 gram of tissue.
India:
India SAR limit is 2 watt per kg . This is same as
ICNIPR guidelines The inter Ministerial Committee of EMF Radiation set up by
the Ministry of Communications and Information Technology had suggested
stricter SAR Limits (1.6 watt per kg) form mobile handsets.
European Union:
CENELEC
specify SAR limits within the EU, following IEC
standards. For mobile phones, and other such hand-held devices, the SAR limit
is 2 W/kg averaged over 10 g of tissue (IEC 62209-1).
For Magnetic Resonance Imaging the limits (described in IEC 60601-2-33)
are slightly more complicated:
|
Averaging time |
6 minutes |
|||||
|
Whole body SAR |
Partial body SAR |
Head SAR |
Local SAR |
|||
|
Body Region |
whole body |
exposed body part |
head |
head |
trunk |
extremities |
|
Operating Mode ↓ |
(W/kg) |
(W/kg) |
(W/kg) |
(W/kg) |
(W/kg) |
(W/kg) |
|
Normal |
2 |
2 - 10 (b) |
3.2 |
10 (c) |
10 |
20 |
|
1st Level Controlled |
4 |
4 - 10 (b) |
3.2 |
10 (c) |
10 |
20 |
|
2nd Level Controlled |
>4 |
>(4 - 10) (b) |
>3.2 |
>10 (c) |
>10 |
>20 |
|
Short term SAR |
The SAR limit over any 10 s period
shall not exceed three times the stated values |
|||||
Notes:
(a) Local SAR is determined over a mass of 10 g.
(b) The limit scales dynamically with the ratio
"exposed patient mass / patient mass":
NORMAL OPERATING MODE: Partial body SAR = 10 W/kg –
(8 W/kg * exposed patient mass / patient mass)
FIRST LEVEL CONTROLLED OPERATING MODE: Partial body SAR = 10 W/kg – (6 W/kg *
exposed patient mass / patient mass)
(c)In cases where the ocular orbit is in the field
of a small local RF transmit coil, care should be taken to ensure that the
temperature rise is limited to 1 °C.
In comparison to the short term, relatively
intensive exposures described above, for long term environmental exposure of
the general public there is a limit of 0.08 W/kg averaged over the whole body.
The SAR for mobile phones is generally in the range
0.5 - 1.5 W/kg.
SAR for electromagnetic energy can be calculated
from the electric field
within the tissue as:
here
Disadvantages of
the SAR technique.
SAR traditionally measures exposure to
electromagnetic fields between 100 kHz and 10 GHz. One problem with SAR is that the value will
depend heavily on the geometry of the part of the body that is exposed to the
RF energy, and on the exact location and geometry of the RF source. For this reason, tests must be made with each
specific source, such as a mobile phone model, and at the intended position of
use. For example, when measuring the SAR due to a mobile phone the phone is
placed at the head in a talk position. Obviously temperature probes can't be
placed inside the human body so phantoms are often used to measure SAR.
Such phantoms contain fluids or gels made up with
electrical conductivities and densities to try and mirror those of the human
body. However, no such fluid or gel is
able to mimic the human body across a substantial frequency range. Also in the human body there are blood
vessels and nerves and layers of different types of tissue as well as internal
organs all of which have their own unique dielectric properties.
Another way of trying to estimate SAR is by
calculation based on Finite Difference Time Domain Methods and a direct
application of Maxwell's equations. The
problem here is whether or not to use a homogenous model where an average
dielectric value for all tissue types
used or whether to use an inhomogeneous model comprising layers and
dividing the body effectively into cubes. This method requires substantial
computing power more so at frequencies less than 50 MHz or greater than 700 MHz
where the 3D cell (voxel) size becomes so small that there are many tens of
thousands of them to be calculated upon.
Further there are substantial differences whether the body is grounded
or not (1). In a practical situation the ground
impedance will highly variable due to clothing, footwear and body position so
any calculations, no matter how complex, will not be of much use.
Another study which has shed light on the use of
SAR's relates to the calcualtion of heating of implantable devices during magnetic
resonance imaging, where it has actually been shown that using only
the whole-body SAR as a recommendation for a safety profile is potentially
dangerous, see Nitz et al 2005 (2).
Christ et al (2006) (3)
identifies two different effects which can lead to increased SAR in layered
tissue in comparison to the SAR assessed using homogeneous tissue simulating
liquid and found for larger distances between the tissue and the antenna,
standing wave effects occur depending on the frequency and fat layer thickness.
This in itself is a pseudo resonance
referred simply to as ‘layering resonance’ which might give pockets of intense heat
absorption at different depths not
unlike that expected due to the notion of quantum mechanical effects proposed
elsewhere, see Barnes ( 4 ). Also in the very close near-field
(distances approximately lambda/40), reactive E-field components lead to high
local absorption in the skin. The latter effect occurs at lower frequencies and
depends on the antenna type. In phantom measurement SAR techniques modification
of the parameters of the homogeneous liquids employed cannot compensate for
these effects. SAR in these cases can be out by up to a factor of 3. Layered
resonance effects involving skin, fat and muscle are known which give resonance
frequencies in the range 400 MHz to approximately 3 GHz.
The final drawback of SAR calculations is that they do not include
magnetic permeability. While magnetic
permeability of tissue is reckoned to be close to that of the vacuum, there are
subtle differences particularly for blood and tissue with a rich blood
supply. The magnetic susceptibility of
blood also changes with oxygenation level.
Human tissue particularly brain tissue, especially hippocampus, has
recently been found to contain nano-particles of
bio-magnetite. The translational
energy of clumps of magnetite exposed to slow time varying fields can exceed
typical covalent bond energies (5).
This could potentially account for some
ELF effects of even quite weak ( milli-Tesla)
magnetic fields or even effects of pulse modulated VHF and UHF radio
signals.
Combining frequency dependent magnetic effects, however small, with
frequency dependent permittivity introduces another level of complexity into
SAR modelling, which has, as far as the present author is aware, never been
attempted.
It would seem then at best SAR is as good as the model used and being an
average gives no notion of potentially dangerous heating at certain biological
interfaces within the body in response to r.f. radiation nor does
it take into account internal resonances however caused. It would seem SAR is presently a comfort
factor for licensors and licensees of mobile and wireless technology and due to
the enormous complexity of the modelling involved SAR may remain for a while to
come yet. One possible thought, thermal
imaging may be a way forward to check RF power deposition. The technique has
been used so far only with respect only to MRI fields see Cline et al 2004 (6).
Resonance
external and internal
The
notion of the Human body having a radio frequency resonant point or points is
not new. Yanase
and Hirate (2011)
(7) calculate effective resistances and resonant frequencies and given the
resistance range of between about 50-400 ohms it seems what they show implies
to the present author that the Human body might act as a remarkably good
antenna in the 40-100 MHz region. This encompasses the original now defunct
Band 1 TV broadcasting band, the 6 and 4 metre Ham Radio Bands and the Band 2
VHF FM broadcasting band. Moving radio
frequency fields of even weak and modest field strengths in this frequency
range have been seen to elicit motor responses of the hands and arms in humans (8-10).
Energy
harvesting implantable bio-chips may be used inside the human body and maintain
a certain resonant Q. Allowing for skin
depth, why then cannot a body internal organ or glands, of dielectric property
substantially different from its surroundings, behave as an independent
dielectric resonator in a similar manner?
Such behaviour has been suggested by the present author elsewhere (4).
For example a good estimate for the resonant frequency of the
prostate gland is 600 MHz. Along similar lines yet at the other end of
the scale is indeed an unusual notion that is that the entire blood volume
could resonate at a frequency much less than that of the body as a whole! The brain might resonate at about 200 MHz. These are
coincidentally all frequencies or close to frequencies used for radio and TV
broadcasting.
Sophisticated
equipment is not needed to prove resonant absorption into human subjects, see
Hatch 2012, Ham Radio Blog(11).
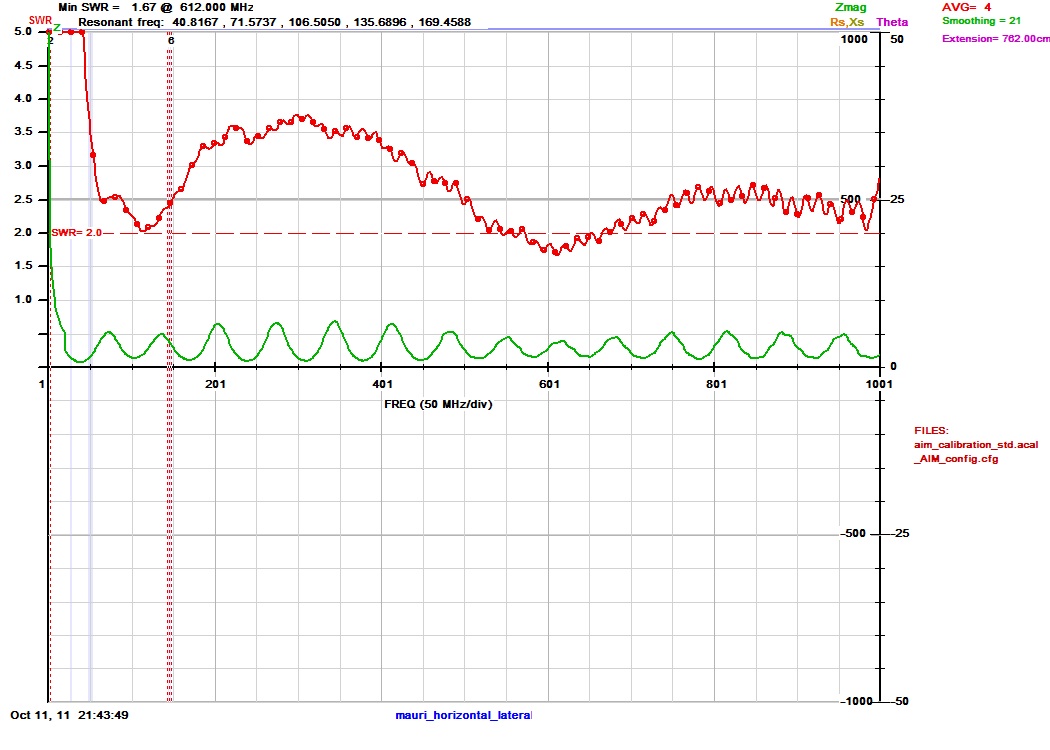
Hatch
has shown by using a direct coupled electrode antenna like system on his own
body that the body has multiple resonances.
In
the above example such resonances are seen at 53,112 and 600 MHz, these are the
points of lowest standing wave ratio in the plot. There is a hint of a minor
response at about 240 MHz as well. It
is almost bizarre that these are all frequencies that either have in the past
or are presently used in the UK for radio or TV broadcasting. The 600 MHz dip is probably due to a
layered resonance effect see above.
Other resonances of separate external body parts so called geometric
resonances of head, arms and legs are also possible and are highly position
dependent.
4G
In
the UK spectrum around 2600 MHz is being or is proposed to be used for 4G. Others are proposing to use some of the spare
former TV spectrum around 600 MHz. Given the findings of Hatch above and the
calculations of Barnes (4) with
regard to the prostate gland and inexplicably rising cases of prostate cancer
in particular (12,13) Thus the view of the present author is that we
really ought to err on the side of caution.
o
o
Safe or not
safe?
o
There exists a simply huge volume of
published work on the effects of r.f. radiation. The
work has covered in vitro- human and animal cell studies, in vivo animal
studies, a few in vivo human studies and epidemiology studies. Many of these studies have focused in on
cancer. Some conclude that RF has no or
little effect while others conclude that RF is a Cancer Promoter rather than a
Carcinogen. Recently the WHO classified
mobile phone radiation as a carcinogen
on the basis of the now famous Glioma study (14).
If RF is a cancer promoter then it is logical to assume under the
correct conditions it would be a general tissue growth promoter and useful in
say wound and bone healing. Thus, not surprisingly, and also recently a new
science, so called PEMF (pulsed electromagnetic field) for bio-medicinal
therapies seems to have evolved with a sudden surge of related PEMF products
available on the market from pain killing devices to local anaesthesia and
wound healing (15,16).
The author has read much of these
works and by way of review personally concludes that for whatever reason with r.f in general, digital pulse and a.m. technologies would
seem to provoke more biological effects than f.m. and
c.w. , particularly with a view to voltage gated effects such as
changing calcium ion efflux (17). As well as in heart and muscle, voltage
gated calcium channels are also found in some cancer cells, see Li and Xiong 2011 and Monteith et al
2012 (18), and play an important
role in cancer progression. For example, T- type Cav
was found in human prostate cancer and up-regulated during neuro-endocrine
differentiation. The L-type calcium
channel subunit has also been found in colon cancer cells. Cav
1.2 expression increases with the differentiation of colon cells to cancer
cells. P- and L- type Cav
have been found in small lung carcinomas. Calcium spikes, which are caused by
unspecified T-type calcium channels and play a role in membrane depolarization,
have been shown to alter the motility of fibrosarcoma
cells.
Since PEMF (pulsed electromagnetic
fields) are used for bone and wound healing clearly they influence cell
division and growth. There are minimal references
in the literature to RF radiation as a cancer inhibitor other than because of
thermal ablation but there are a couple of notable exceptions on is (Kalantaryan et al 2011 ) (19) who describe low level coherent
millimetre wave radiation as an inhibitor of certain cultured cancer cells in
vitro. The other is an animal model cancer study of Berg et al 2010 (20) which talks of 50 Hz PEMF and SEMF
at 15-20 mT
level applied by a solenoid coil.
This is exactly the level of field that is suggested to cause magnetite
cluster translational energies to be of the order of those of covalent
bonds. Ion cyclotron resonance effects
are yet another possibility. The author
has suggested elsewhere that only with a quantum mechanical explanation can we
properly understand the benefits and risks of r.f
radiation in general. This in the
author’s opinion is borne out exceeding well by Smith’s reappraisal of the
Sutton Coldfield TV Transmitter Cancer Cluster Study (21). The author has
recently created predictive algorithms to show the most dangerous positions for
humans and vegetation alike in the proximity of transmitter antennas. When quantum mechanical concepts are
employed, Bayesian statistics will be required to understand geographical
effects in epidemiological studies.
Another reason why epidemiological studies don’t always produce expected
results is that RF exposure depends on people’s position and mobility. In the author’s opinion sleeping position
and mattress type may also be critical factors.
Conclusions
The shortcomings of present SAR
techniques have been highlighted. Given skin/fat/muscle layering resonances,
the resonant frequency and position of the prostate gland (as a dielectric
antenna) and
the proposals for 4G in the UK, the author really feels we should be erring on
the side of caution. Based on the
available evidence the present view of the author is that RF radiation under
most conditions is very probably not a carcinogen but is capable of either
accelerating or inhibiting cellular growth.
So if you have a genetic or environmental predisposition and some early
stage cancer cells, possibly some very
specific RF frequencies and intensities could potentially speed up their
division and growth. Based on this we
should perhaps carefully review our choices of frequency bands in the
future. Human beings evolved prior to
synthetic RF but evolved bathed in the earth’s natural field, exposed to DC and
slow time varying magnetic fields, Schuman Resonance, Auroral
and Meteor signals and solar and galactic generated microwave bursts. Thus
human beings are indeed ‘beings of frequency’ this has been recognised in the
last century by some the worlds’ greatest of physicists such of Frolich (22) and
Herbert Pohl (23). More recently Smith (24) and Kirshvink (25) have added to the understanding of ‘electromagnetic man’ and
indeed all have inspired the present author’s some would say radical (or at the
very least diverse) thought in this area.
Today we exploit RF for body scanning in MRI and thermography. RF can also be used rather indiscriminately
in certain forms of thermotherapy or cellular ablation treatment. Low energy PEMF has been regarded by some as
almost ‘quackery’ but there is growing evidence that if the frequencies and
PRFS are appropriate then it does indeed work (26).
Cellular autonomic behaviour has
recently shown to be fractal (27). A new design in antennas using fractal
concepts shows multi-specific frequency behaviour (28). One day we link these
two concepts and living beings will no longer be in any danger of external
electromagnetic fields for the fields we use will be appropriately chosen and
tuned for our protection and indeed even our benefit and indeed some will perhaps
by means of voltage reflection measurement become our diagnosticians and our
healers conjuring up a vision of Science Fiction’s star trek and Bone’s ‘tricorder’ device (29). Application of such fields either by external
antenna making use of new geometric attenuation principles (4) to dump scalar energy or
by injectable
tiny rf devices might one day be used to time reverse our
tired cells a sort of electromagnetic elixir of youth if you will. Such devices are already so small they can
be swallowed e.g. radio pills (30). It is imagined that just as we on the verge
of understanding disease at the genetic and molecular level and designing
designer drugs tailored to an individual’s particular genetic makeup hand in
hand will they will eventually be given their ideal complimentary quanta of
electromagnetic energy as well.
References
1. Hirata et
al 2012. http://www.ncbi.nlm.nih.gov/pubmed/23202273
2. Nitz et al 2005. http://www.ncbi.nlm.nih.gov/pubmed/16304480
3. Christ et
al 2006. http://iopscience.iop.org/0031-9155/51/19/014
4. Barnes
2013. http://www.drchrisbarnes.co.uk/RFEM.htm
5. Strbak et al
2011. http://www.measurement.sk/2011/Strbak.pdf
6. Cline et
al 2004. http://www.ncbi.nlm.nih.gov/pubmed/15170832
7. Yanase and Hirata 2011. http://www.jpier.org/PIERB/pierb35/02.11082511.pdf
8. Huttunen
et al 2009 http://www.pathophysiologyjournal.com/article/S0928-4680(09)00010-8/abstract
9. Huttunen
et al 2011 http://www.ncbi.nlm.nih.gov/pubmed/21616774
10. Huttunen
2012 http://herkules.oulu.fi/isbn9789514297601/isbn9789514297601.pdf
11. Hatch
2012,
Ham Radio Blog
12. news.google.com/newspapers?nid=1988&dat=19930817&id...
13.
articles.latimes.com/2003/aug/22/local/me-cancer22
14. http://www.iarc.fr/en/media-centre/pr/2011/pdfs/pr208_E.pdf
15.
http://www.painsolv.co.uk/207-210-196/PEMF_Explained
16. http://www.pulsed-electromagnetic-therapy.com/pemf-science/
17. http://www.qub.ac.uk/research-centres/nicr/FileStore/Filetoupload,25239,en.pdf
18. Monteith et al http://www.jbc.org/content/early/2012/07/20/jbc.R112.343061.full.pdf
19. Kalantaryan et al
2011 http://www.jpier.org/PIERL/pier.php?paper=10110806
20. Berg
et al 2010 http://www.pemfnow.com/wp-content/uploads/2012/10/PEMF_painfibrocancer_sm.pdf
21. http://cwl2004.powerwatch.org.uk/programme/posters/day4-smith.pdf
22. http://link.springer.com/chapter/10.1007/978-1-4613-2105-7_8#page-1
23. Pohl
1980, ‘Natural electrical r.f. oscillation from
cells’ http://link.springer.com/article/10.1007%2FBF00763837#page-1
24. "Electromagnetic Man," Cyril W. Smith and Simon ... C.W. Smith, R.Y.S. Choy and J.A. Monro, 1989
25. Magnetite
in Human Tissues: A Mechanism for the Biological Effects of Weak ELF Magnetic
Fields- http://web.gps.caltech.edu/~jkirschvink/pdfs/KirschvinkBEMS92.pdf
26. http://www.imtc.co.il/bio/wp-content/uploads/2012/05/4_-Strauch_PEMF_Aesthetics_2009_sm.pdf
27. http://www.nature.com/news/2009/090904/full/news.2009.880.html
28. http://esjournals.org/journaloftechnology/archive/vol3no3/vol3no3_3.pdf
29. http://en.wikipedia.org/wiki/Tricorder
{kind=link}